Introduction
Reflecting the trend observed in other European countries, there has been a steady increase in IVF provision in Ireland in recent years [1,2]. Perhaps because IVF was initially undertaken by a limited number of Irish patients, having a statutory framework addressing assisted human reproduction (AHR) treatments in Ireland was not an immediate priority among national health policy goals. The need for Irish governmental oversight and a comprehensive legislative structure regarding AHR was formally recognised in 2001 with the establishment of the Commission for Assisted Human Reproduction (CAHR). This expert panel was charged with exploring possible regulatory approaches for assisted fertility treatment in Ireland. More specifically the CAHR Terms of Reference included publishing "a report on the possible approaches to the regulation of all aspects of AHR and the social, ethical and legal factors to be taken into account in determining public policy and in this area." The 151-page CAHR report was released in 2005 [3].
Of note, the Commission's first recommendation was a call for a regulatory body to be "established by an Act of the Oireachtas to regulate AHR services in Ireland". Such an agency would advise government on all matters concerning AHR and associated procedures including research in Ireland. Yet, since the CAHR report was published in 2005 there has been no progress towards legislation-although the topic does still occasionally receive attention during parliamentary debate [4]. Some legislators are mindful of this regulatory void, and acting Seanad leader Ivana Bacik regretted that questions about AHR in Ireland had to be confronted on a case-by-case basis (i.e., by judicial channels): "Indeed, it's unfair on couples, on parents and on families to have to take litigation. Many of us have been saying this for years. We need legislation on IVF, on assisted human reproduction and on surrogacy" [5].
Having no AHR legislation in Ireland means that the only guidance medical practitioners have concerning clinical assisted fertility comes from the Irish Medical Council, in the form of its Guide to Professional Conduct & Ethics for Registered Medical Practitioners. This guidance on AHR from the Medical Council has undergone considerable change in recent years and these policy modifications occurred during a time when the composition of the Council was also reconfigured [6]. The present study sought to reappraise Irish public opinion on AHR, to assess any changes in public opinion compared to nearly a decade previously.
Methods
A multidisciplinary team of physicians, nurses, and demographers developed a brief questionnaire (validated externally by a private polling firm) to measure public opinion on multiple aspects of AHR. Unlike the CAHR study, this research was funded from our clinic budget and received no government support. Data were obtained by landline and mobile telephone, using random digit dial methodology whereby all households in Ireland (including unlisted numbers) remained eligible for sampling. Interviews were anonymous and no personally identifiable information was collected to ensure respondent confidentiality (no in-person contact was made). Each respondent was sampled only once; all polling was conducted in March 2013. Data were tabulated by professional canvassing staff (Red C Marketing & Research Ltd., Dublin, Ireland) using a computer aided telephone interviewing (CATI) modality. The CATI approach has a documented non-response rate of about 6% as validated by prior electoral and social queries, and this sampling technique produces some of the most accurate polls in Ireland. For example, during the 2011 campaign for the President of Ireland a national sample of about 1,000 predicted the election outcome to within 0.7% of the final ballot tally [7,8].
The following demographic parameters were queried: age, gender, geographic location, socioeconomic status, whether or not the respondent had any children (and if yes, how many), and whether or not the respondent had experience with AHR treatment (or had contemplated seeking such treatment). Next, respondents were asked the following questions: "With regard to fertility treatments such as IVF, do you agree or disagree that the government should pass legislation to deal with these treatments in Ireland? Do you agree or disagree that any fertility services now available internationally should also be available in Ireland? Would you be in favour or against allowing these services in Ireland: IVF, sperm donation, egg donation, embryo donation, pre-implantation genetic diagnosis, or embryo sex-selection during IVF? Thinking about if the government were to make laws regarding egg and sperm donation, please give your opinion on how the anonymity of the donor should be addressed: donation where the donor consents to being involved in the future life of any child born from that donation, donation where the donor agrees to be contacted by any child born of any donation, identifiable donation where the donor agrees to have their identity made available to the child after he/she reaches 18 years of age, or anonymous donation where the law completely protects the privacy of the donor. If egg and sperm donation were to be legislated for in Ireland, it has been suggested that anonymous donation would be banned and any child conceived from egg or sperm donation would have a right to know who the donor was. To what extent do you support this suggestion?"
Responses were tabulated on a five-point Likert scale, ranging from 1, strongly oppose; 2, slightly oppose; 3, neutral/no opinion; 4, slightly favour; and 5, strongly favour.
Mathematical models were used to define quotas allowing equal survey input on the basis of age, gender, socioeconomic class, and geographical region. The sampling methodology statistically captures a representative sample of 98% of the adult Irish population (i.e., age ≥18). Modified National Readership Survey definitions were used for class designation, as follows: A, upper middle class (higher managerial, administrative, or professional); B, middle class (intermediate managerial, administrative, or professional); C1, lower middle class (supervisory or clerical, junior managerial, administrative or professional); C2, skilled working class (skilled manual workers); D, working class (semi-skilled & unskilled manual workers); E, those at lowest level of subsistence (pensioners, widows, casual or lowest grade workers); and F, unemployed [9]. The project was submitted to an independent ethics board, but because this was a survey of the general population and because no identifiable clinical data were recorded, the research was classified as exempt from review.
Results
The questionnaire was completed by 1,003 individuals between 18th-20th March 2013; 49% were female and 51% were male (age range, 18 to "65 or over"). A social status of either A, B, or C1 was reported by 41% of individuals, while 59% were either C2, D, E or F. Of the 37% sample with no children, 42% were male and 44% were resident in Dublin. The average number of children in the overall sample population was 1.84. Of the 6% with infertility experience, only half (3%) had undertaken therapy with the remainder (3%) having researched (but not initiated) treatment.
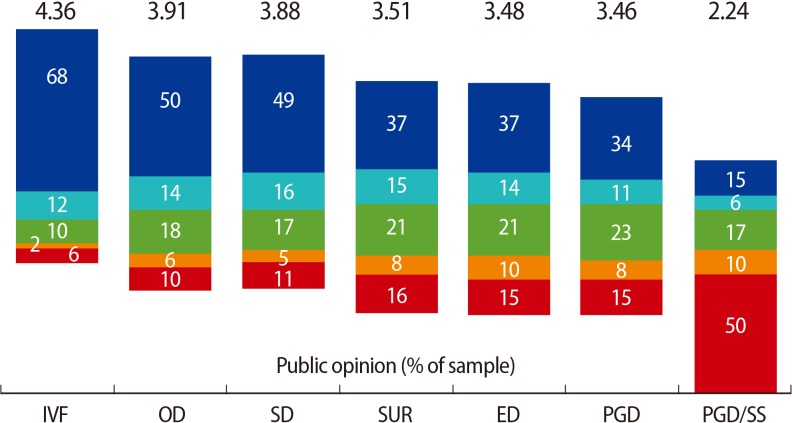
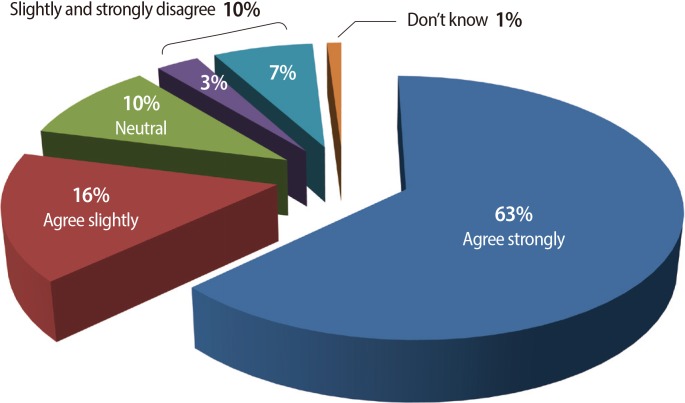
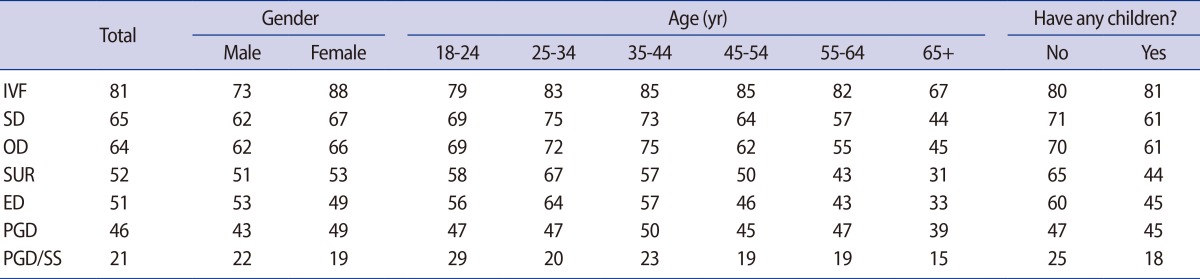
Agreement was high that, in principle, any fertility services offered in other countries should also be available in Ireland. Support for this did vary as a function of specific AHR intervention, as shown in Figure 1. Age, gender, child status, social class, and geographic distribution among those favouring each type of AHR treatment in Ireland are presented in Tables 1, 2. Regarding donor gamete treatment in Ireland, 80% favoured treatment involving identifiable donation (where the donor agrees to have their identity made known to the child after s/he reaches age 18). Subgroup analysis showed support for this policy to be highest among those respondents aged 18 to 24, and among those with no children. Donation where the donor agrees to be contacted by the child born following donation, and anonymous donation where donor privacy is completely protected by law were supported by 68% and 66%, respectively. The least popular (53%) donor gamete treatment type appeared to be donation where the donor consents to be involved in the future life of any child born as a result of donor fertility treatment. Respondents in social class ABC1 (58%), age 18 to 24 (62%), age 25 to 34 (60%), or without children (61%) were more likely to favour this donor treatment policy in this sample. Concerning the need for legislation covering fertility services in Ireland, most (79%) respondents favoured government involvement (Figure 2).
Discussion
The lack of Irish legislation on AHR has become more problematic as the number of patients seeking fertility treatments in Ireland has increased, resulting in an intractable health policy puzzle of expanding dimensions [10-12]. Recent research has explored selected aspects of AHR in Ireland including compensation for IVF gamete donors and their privacy [13], embryo disposition [14] and abandonment of IVF embryos in Ireland [15]. While these reports did yield original information, the findings were limited because they were based on data derived only from individuals already seeking medical fertility consultation. The present study brings questions concerning AHR before a national Irish audience, and is the first such sampling undertaken without government sponsorship or oversight.
Our survey data show that 94% of the general Irish population has no personal experience with any medical fertility therapy. Nevertheless, public support for IVF remained above 50% even among individuals age 65 or older. This is a previously unreported observation; it suggests a willingness by Irish senior citizens to support a class of treatment which the respondents themselves would not seek personally. It would be reasonable to expect an even higher level of support for AHR interventions if our investigation had been confined only to the subset of Irish adults with direct infertility experience, and this represents the focus of additional research.
Donor gametes in assisted fertility treatment have long been a source of debate, particularly on the matter of privacy and confidentiality, and there is no consensus among policy experts and ethicists as to what represents the best way forward [16,17]. The relevance of donor oocyte policy in Ireland thus far has been limited, because just one Irish IVF unit provides this service [18]. This investigation shows mixed public opinion on oocyte donation in Ireland, with most respondents favouring identifiable donation. In this sample, public support was lowest for AHR treatments where the gamete donor was allowed to be involved in the life of the offspring. This finding generally aligns with previously published questionnaire data collected in Dublin from IVF patients themselves [19].
From these data, most respondents (77%) appear to agree in principle that any fertility treatment offered internationally should also be available within Ireland. IVF is the best known of the advanced reproductive technologies, and it was viewed positively by most of the Irish public sampled. However, we registered progressively reduced public support of sperm donation, oocyte donation, and embryo donation, surrogacy, pre-implantation genetic diagnosis (PGD) and embryo sex-selection in Ireland. While our research did identify broad public support for most types of AHR treatment in Ireland, embryo sex-selection was the exceptional case, with half of the sample expressing a strongly negative opinion of this particular fertility service.
Our study has several potential limitations which should be considered. Although sampling adequacy can be a concern in any national survey, the statistical model used by an experienced polling group is regarded as robust. Unfortunately, it was not possible to make matched comparisons to the original CAHR assessments because the Commission did not publish raw polling data from 2001 to 2005. There is also the fundamental question of how well complex AHR treatments are actually understood in the general community (where most have no direct experience with infertility or its possible treatments). Particularly for PGD, even among some physicians the knowledge level of advanced genetic tests can be low [20]. However, because these data were gathered by professional staff experienced in sampling Irish public opinion on other complex and sensitive topics (i.e., abortion, education funding, immigration, tax policy, etc.), we believe our results involve very little bias.
In conclusion, results from this contemporary national sample provide new evidence that most Irish citizens support this government in legislating for IVF and allied treatments. IVF is not currently provided by the Irish public health service, nor was this benefit available in the past. Most respondents will never require AHR treatment themselves but still appear to support clinics in Ireland offering the same assisted fertility treatments that are available internationally. These views remain largely consistent with the CAHR recommendations from 2005. Only on matters of embryo sex-selection and gamete donor privacy were specific CAHR recommendations found lacking in current support, although further research is needed to clarify exactly how popular opinion on these issues has changed. It appears that legislation allowing for the full range of donation options (and not mandating disclosure of donor identity at a stipulated age) would better align with contemporary Irish public opinion. Although our data show the population of Ireland does not support PGD for elective sex-selection, it is possible that the application of this technology with IVF would be accepted if limited to the prevention of serious sex-linked genetic conditions. These issues represent the focus of ongoing research at our institutions to better inform the wider public discourse on AHR regulation in Ireland.