Efficacy of intralipid administration to improve in vitro fertilization outcomes: A systematic review and meta-analysis
Article information

Abstract
We performed a systematic review and meta-analysis to evaluate whether intralipid administration improved the outcomes of in vitro fertilization. Online databases (PubMed, Cochrane Library, Medline, and Embase) were searched until March 2020. Only randomized controlled trials (RCTs) that assessed the role of intralipid administration during in vitro fertilization were considered. We analyzed the rates of clinical pregnancy and live birth as primary outcomes. Secondary outcomes included the rates of chemical pregnancy, ongoing pregnancy, and missed abortion. We reviewed and assessed the eligibility of 180 studies. Five RCTs including 840 patients (3 RCTs: women with repeated implantation failure, 1 RCT: women with recurrent spontaneous abortion, 1 RCT: women who had experienced implantation failure more than once) met the selection criteria. When compared with the control group, intralipid administration significantly improved the clinical pregnancy rate (risk ratio [RR], 1.48; 95% confidence interval [CI], 1.23–1.79), ongoing pregnancy rate (RR, 1.82; 95% CI, 1.31–2.53), and live birth rate (RR, 1.85; 95% CI, 1.44–2.38). However, intralipid administration had no beneficial effect on the miscarriage rate (RR, 0.75; 95% CI, 0.48–1.17). A funnel plot analysis revealed no publication bias. Our findings suggest that intralipid administration may benefit women undergoing in vitro fertilization, especially those who have experienced repeated implantation failure or recurrent spontaneous abortion. However, larger, well-designed studies are needed to confirm these findings.
Introduction
Although in vitro fertilization (IVF) has come a long way, the success rate of IVF is still less than 40% [1]. Furthermore, approximately 10% of women who receive IVF with intracytoplasmic sperm injection experience repeated implantation failure (RIF) [2]. RIF is generally defined as three cycles of IVF that are unsuccessful even though 1–2 good-quality embryos are transferred in each cycle [3]. Impaired endometrial receptivity has been suggested as a major cause of RIF, and immune abnormalities reduce endometrial receptivity and consequently prevent implantation. Immune abnormalities have also been reported as the cause of recurrent spontaneous abortion (RSA) [4]. Therefore, many immunotherapies have been explored to improve endometrial receptivity and increase the pregnancy rate. Immunotherapy methods suggested for immune dysfunction include leukocyte immunization, intravenous immunoglobulin (IVIG), low-molecular-weight heparin, and intralipid [5,6].
Intralipid, which refers to a lipid emulsion comprising soybean oil, is an example of immunotherapy. Because intralipid is a source of fat, it has traditionally been used as a nutritional supplement for patients unable to eat orally. In addition to its nutritional role as an energy source, intralipid has biological functions, including immune function [7]. Although the immunological mechanism of intralipid is not fully understood, several studies have reported that its active component, soybean oil, inhibited the cytotoxic activity of natural killer (NK) cells [8,9]. Increased NK cell cytotoxicity has been associated with RSA and RIF [10,11]. In this context, many studies have explored the use of intralipid for women with/without RIF or RSA undergoing IVF [12-16]. However, the results of these studies have proven inconsistent and controversial. Therefore, the effectiveness of intralipid administration in infertile women undergoing IVF has not been conclusively established.
In view of the conflicting results of prior studies, we performed a systematic review and meta-analysis to evaluate the effect of intralipid administration on infertile women during IVF.
Methods
We followed the guidelines of the Cochrane Handbook for Systematic Reviews and preferred reporting items for systematic reviews and meta-analyses (PRISMA) checklist protocol. This study protocol was registered with PROSPERO (CRD42020201739).
1. Eligibility criteria
Only randomized controlled trials (RCTs) evaluating whether administration of intralipid plays a beneficial role in women undergoing IVF were considered. We included both published RCTs and unpublished RCTs and searched abstracts presented at major infertility conferences to identify any unpublished trials. Non-randomized studies were excluded from the current meta-analysis due to the high risk of bias. As the crossover design is invalid, these trials were also excluded. The target population was infertile women who had undergone IVF. We measured the rates of clinical pregnancy (CPR) and live birth (LBR) per randomized woman as the primary outcomes. Clinical pregnancy was determined based on the presence of a gestational sac and detectable fetal heartbeat. Live birth was defined as delivery of a live neonate after 24 weeks of gestational age. Secondary outcomes included the rates of ongoing pregnancy (defined when the pregnancy reached ≥12 weeks of gestation) and missed abortion (defined as the intrauterine death of a fetus occurring before 20 weeks of gestational age) per randomized woman. We also assessed adverse events, including adverse reactions to intralipid administration and congenital anomalies.
2. Search methodology for literature identification
We searched online databases including PubMed, Medline, Embase, and the Cochrane Library for all relevant papers through March 2020. The following Medical Subject Headings (MeSH) and text terms were used to retrieve all relevant literature: “intralipid” and (“in vitro fertility” or “IVF” or “assisted reproductive techniques” or “ART” or “repeated implantation failure” or “RIF” or “recurrent pregnancy loss” or “RPL” or “recurrent miscarriage” or “recurrent spontaneous abortion” or “RSA”). There was no language restriction. Studies were independently identified by EJH and SWL.
3. Study selection and data extraction
Initially, two review authors (EJH and SWL) identified potentially relevant trials, and the retrieved titles and abstracts were then screened. We retrieved the full texts of all potentially eligible articles, and both authors (EJH and SWL) independently read through the full-text articles to determine whether they met the inclusion criteria and selected studies for inclusion in the review. Any disagreements regarding study eligibility were resolved by discussion or arbitration by a third author (WSL). The selection process was presented in a PRISMA flow chart.
4. Assessment of risk of bias in the included studies
Two review authors (EJH and SWL) independently evaluated the risk of bias in individual articles using the Cochrane Risk of Bias tool presented in the Cochrane Handbook for Systematic Reviews of Intervention (www.training.cochrane.org/handbook). They evaluated the following seven sources of bias: (1) random sequence generation (selection bias); (2) allocation concealment (selection bias); (3) blinding of participants and personnel (performance bias); (4) blinding of outcome assessment (detection bias); (5) incomplete outcome data (attrition bias); (6) selective reporting (reporting bias); and (7) other sources of bias (other bias). We summarized the results of the risk of bias assessment for the included studies in graphs.
5. Statistical analysis
We conducted the meta-analysis using the RevMan 5.3 software package (Cochrane Collaboration, Oxford, UK). The risk ratios (RRs) with 95% confidence intervals (CIs) for binary data variables were calculated using the Mantel-Haenszel method. Using the I2 statistic to assess the statistical heterogeneity across the included articles, we determined that statistical heterogeneity was absent when I2 was <50%. In selecting the effect models, I2 was used as the standard (fixed model: I2 <50%, random-effect model: I2 ≥50%). We used a forest plot to graphically present the heterogeneity of the treatment effects. Publication bias was also estimated using funnel analysis and the Egger test. Forest plots were generated to present the results of the meta-analysis. When sufficient studies were available, we carried out further analyses within the following subgroups: (1) women without RIF or RSA versus women with RIF or RSA, and (2) women with previous implantation failure versus women with RSA. We also planned sensitivity analyses to evaluate whether our outcomes would have differed if (1) a random-effect model had been adopted, or (2) we had restricted the analysis to only published studies.
Results
1. Study selection and characteristics
In total, 180 articles were collected from electronic databases. Of these, 149 studies were considered ineligible as screening of the titles and abstracts revealed they did not meet the inclusion criteria. After reviewing the full texts of the remaining 31 studies, 26 studies were excluded for the following reasons: 10 studies were non-RCTs, nine studies were reviews, and seven studies reported no relevant comparisons or outcomes. Finally, five RCTs involving a total of 840 patients were included in the present meta-analysis [12-14,17,18]. The search results were presented in a PRISMA flow chart (Figure 1).
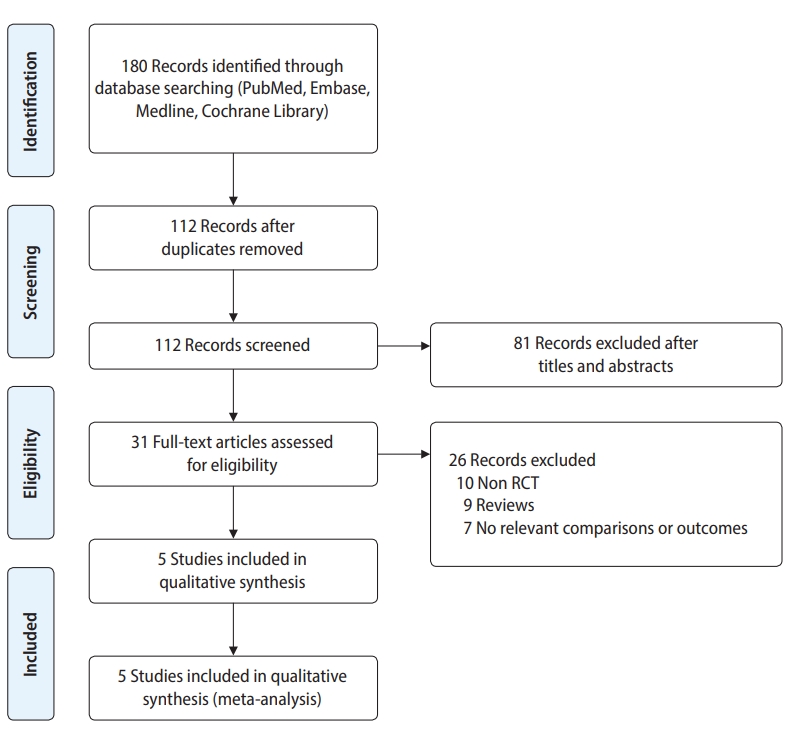
Preferred reporting items for systematic reviews and meta-analyses flow diagram of study selection. RCT, randomized controlled trial.
Three of the included trials were published as full articles [12-14], and two were published as conference abstracts [17,18]. Three studies evaluated the effects of intralipid administration on RIF [12,17,18], one study investigated the influence of intralipid administration on RSA in patients with elevated NK cell levels (>12%) [13], and one study assessed the efficacy of intralipid for infertile women who experienced implantation failure more than once [14]. Most studies excluded women with an abnormal uterine cavity (i.e., endometrial polyp, submucosal myoma, or arcuate uterus). The method of intralipid administration varied among the included trials. In most studies, 20% intralipid was administered twice intravenously. For the first dose, intralipid was infused on the fourth to ninth day of controlled ovarian hyperstimulation [17], the day of ovum pick-up [13,14], or the day of embryo transfer [12]. The second dose of intralipid was administered on the day of embryo transfer [14], the day of the pregnancy test [12], or within 1 week of a positive pregnancy test [13,17]. All five included trials reported the CPR and LBR as outcomes. The chemical pregnancy rate was reported in two trials [13,14], the ongoing pregnancy rate was reported in two trials [13,14] and the miscarriage rate was reported in two trials [12,13]. Table 1 shows the characteristics of the five included studies.

Characteristics of the included studies
2. Methodological quality of the included studies
Most of the included trials had a relatively low to moderate risk of bias according to the guidelines of the Cochrane Collaboration (Supplementary Table 1). We present the outcomes of the risk of bias assessments for the included studies in figures (Supplementary Figures 1 and 2).
3. Outcome measures
1) Clinical pregnancy rate
All five included RCTs (840 patients) reported the CPR. All five RCTs showed that the CPR was higher in the intralipid group than in the placebo group, but the results were statistically significant in only two RCTs [14,17]. Pooling of the data showed a significant improvement in the CPR in the intralipid group when compared with the control group (RR, 1.48; 95% CI, 1.23–1.79; p=0.13). Heterogeneity was not found among the trials, as judged by the I2 value (45%). Thus, we selected a fixed-effect model (Figure 2A).
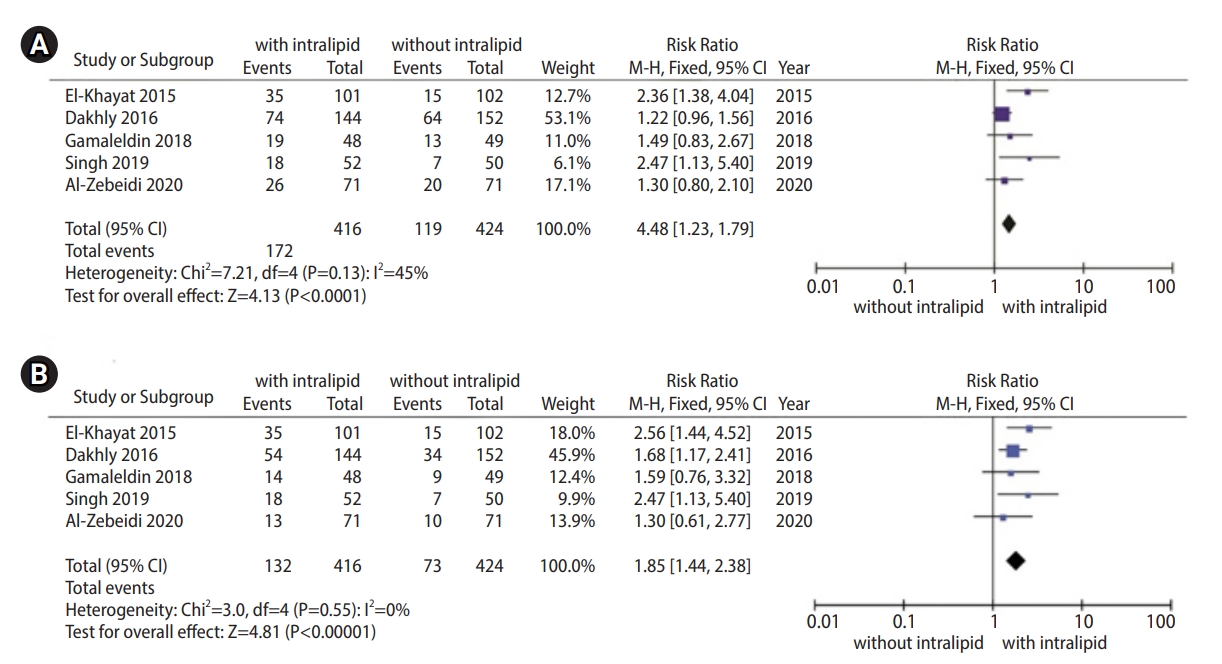
Meta-analysis of the clinical pregnancy rate (A) and live birth rate (B). M-H, Mantel-Haenszel; CI, confidence interval.
2) Live birth rate
All five included RCTs (840 patients) were eligible for inclusion in the meta-analysis of the LBR. In three of the five RCTs, it was confirmed that intralipid significantly increased the LBR when compared to the placebo group [13,14,17]. The RR for the LBR was 1.85 (95% CI, 1.44–2.38) in favor of intralipid administration for infertile women undergoing IVF. Homoge-neity was found among the five RCTs according to the I2 value (0%). According to the result of I2, we analyzed the data using a fixed-effect model (Figure 2B).
3) Ongoing pregnancy rate
Two trials (398 patients) assessed the ongoing pregnancy rate [13,14]. Both studies noted that the rate of ongoing pregnancy in the intralipid group was significantly higher than that in the placebo group. The results of the meta-analysis showed a higher ongoing pregnancy rate when intralipid was administered (RR, 1.82; 95% CI, 1.31–2.53; p=0.38). When the I2 statistic was calculated, no heterogeneity was identified (I2=0%). We performed the meta-analysis using a fixed-effect model because I2 was <50% (Figure 3A).

Meta-analysis of the ongoing pregnancy rate (A) and miscarriage rate (B). M-H, Mantel-Haenszel; CI, confidence interval.
4) Miscarriage rate
The miscarriage rate was reported in two RCTs with 438 patients [12,13]. One of them showed that intralipid significantly decreased the miscarriage rate when compared to the control group [13]. Pooling of the data revealed no beneficial effect of intralipid injection on the miscarriage rate (RR, 0.75; 95% CI, 0.48–1.17; p=0.21). Homogeneity between the two RCTs was identified using the I2 statistic (22%). Thus, we selected a fixed-effect model (Figure 3B).
5) Adverse events
Four of the included studies assessed adverse events, which did not show a statistically significant difference between the intervention group and control group [12-14,18]. In two of these trials [14,18], one congenital diaphragmatic hernia and two congenital external ear anomalies were reported in the intralipid treatment groups. In the other trials [12,13], no adverse events of intralipid administration were reported.
4. Publication bias analysis
The five RCTs included in this meta-analysis were evenly distributed across the graph in the funnel plot analysis, showing no publication bias (Figure 4).
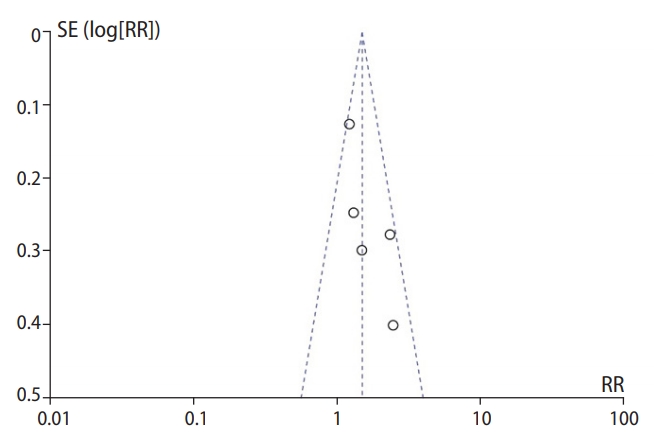
Funnel plot comparison showing publication bias. SE, standard error; RR, risk ratio.
5. Subgroup analysis and sensitivity analysis
We did not conduct a subgroup analysis since it was not possible to extract data for populations without RIF or RSA. In a subgroup analysis of women with previous implantation failure versus women with RSA, we found higher CPR and LBR for women with previous implantation failure, and the pooled RRs were 1.74 (95% CI, 1.27–2.40) and 1.98 (95% CI, 1.39–2.80), respectively (Supplementary Figure 3). For women with RSA, only one study was reported, according to which LBR improved compared with placebo or no treatment (Supplementary Figure 3). Sensitivity analyses using a random-effect model or limited to only published studies did not result in different conclusions regarding the CPR, LBR, ongoing pregnancy rate, and miscarriage rate (Supplementary Tables 1 and 2).
Discussion
This meta-analysis was conducted to evaluate the effectiveness of intralipid administration for infertile women undergoing IVF. Five RCTs involving a total of 840 infertile women were included. The meta-analysis showed that IVF outcomes, including the CPR, ongoing pregnancy, and live birth, improved when intralipid was used as an adjunct treatment in women undergoing IVF, especially for RIF or RSA.
The current review showed that intralipid administration improved the LBR compared with the control group (RR, 1.85; 95% CI, 1.44–2.38) (Figure 2B). This finding is consistent with the preliminary results of a meta-analysis presented by Asif et al. [19] at the 34th Annual Meeting of the European Society of Human Reproduction and Embryology (RR, 2.13; 95% CI, 1.35–3.36). This review provided more reliable evidence because it analyzed more participants than the study of Asif et al. [19] (5 RCTs with 840 participants vs. 2 RCTs with 303 participants). Another difference relates to the inclusion criteria, as the authors [19] included only women with RIF, whereas this review included women with RSA as well as RIF, because intralipid is known to effective in suppressing NK cytotoxicity which has been suggested as a common cause of RIF and RSA.
Although not included in this meta-analysis, we did find non-RCTs assessing the effects of intralipid on IVF outcomes. Martini et al. [16] evaluated the effects of intralipid infusion on 127 women with RIF or RSA who had elevated NK cell levels (≥19%) and had undergone assisted reproductive technology (IVF or intrauterine insemination). They administered intralipid (4 mL of 20% intralipid diluted in 250 mL of normal saline) 7–10 days before embryo transfer or insemination, a second dose at a gestational age of 6 weeks and again at a gestational age of 10 weeks. In that study, intralipid failed to improve the CPR or LBR when compared with the baseline rates published by Tang et al. [20] (p=0.12 and p=0.80, respectively). The use of historical control data was a notable limitation of this study. Another non-RCTs assessing the utility of intralipid in infertile women with RIF or RSA was reported by Check and Check [15]. They analyzed the effect of intralipid in a more specific patient group (aged 40–42 years) compared to the patient groups of the studies included in our meta-analysis. Intralipid (4 mL of 20% intralipid diluted in 100 mL normal saline) was infused during the mid-follicular phase. The authors demonstrated that intralipid did not increase the LBR in infertile women undergoing IVF who experienced RIF or RSA (p=0.087). The differences between these findings and those of our meta-analysis may be due to the different study populations. The efficacy of intralipid in women of advanced reproductive age with RIF or RSA should be evaluated in further studies.
The immune mechanism of intralipid has not been fully identified, but several previous studies have suggested that it has immunosuppressive properties that inhibit NK cytotoxic activity and production of pro-inflammatory cytokines such as tumor necrosis factor-alpha, interleukin-6, and interleukin-8 [8,9,21]. In particular, NK cytotoxicity has been suggested as a cause of RIF and RSA [10,11]. It has been shown that intralipid affects NK cells through receptors such as the G protein-coupled receptor and peroxisome proliferator-activated receptor (PPAR) [22-25]. The fatty acids in intralipid and its metabolites act as ligands that activate PPAR expressed in NK cells. PPAR activation reduces NK cytotoxicity and consequently enhances implantation and maintains pregnancy [26-29]. PPAR also plays an important role in implantation, invasion of cytotrophoblasts, embryo growth, and formation of the placenta [25,30].
Like intralipid, IVIG is also effective in suppressing NK cytotoxicity [29,31] and has been used successfully to treat RIF and RSA. However, IVIG is expensive and is associated with side effects such as transfusion-transmitted diseases because of a blood product. In recent years, some authors have suggested that intralipid and IVIG are equally effective in decreasing NK cell cytotoxicity. Coulam and Acacio [32] compared the effects of intralipid and IVIG in infertile women who had experienced reproductive failure and increased NK cell levels (n=442). There were no significant differences between the intralipid group (n=200) and IVIG group (n=242) in the LBR or ongoing pregnancy rate (61% vs. 56%, respectively). In 2016, Meng et al. [10] conducted an RCT to compare the effects of intralipid (n=78) and IVIG (n=78) in women with unexplained RSA and elevated NK cell levels (>20%). The authors noted that the successful pregnancy rates of the two groups were similar (92.1% vs. 88.2%; p=0.415). These data suggest that intralipid is sufficiently effective and may be used as an alternative to IVIG for the treatment of RSA or RIF. Furthermore, intralipid is less expensive than IVIG. However, RCTs with larger sample sizes are needed to confirm that intralipid and IVIG are both effective treatments for RIF or RSA.
To ensure quality, we included only RCTs in the meta-analysis. Furthermore, selection bias was reduced, as two reviewers independently selected the trials and extracted the data. There were also several limitations to our review. One was the heterogeneity of the included trials. There were differences among the study populations (infertile women with RIF, RSA, or a history of implantation failure). There was also variability among the intralipid administration protocols in terms of dose, frequency, and duration. Therefore, the optimal dose, frequency, and duration of intralipid were not confirmed. Another limitation is that only a small number of studies were included in the meta-analysis. Despite these limitations, the present meta-analysis provides clinicians with a meaningful summary of the existing studies on the effectiveness of intralipid for infertile women undergoing IVF with RIF or RSA.
In conclusion, the findings of the current meta-analysis and systematic review suggest that intralipid administration may improve IVF outcomes, especially in women with RIF or RSA. However, due to some limitations of this review, intralipid in women undergoing IVF should be used with caution and these findings need to be further evaluated in larger, well-designed studies. The mechanisms and safety of intralipid and the optimal protocol for intralipid administration should also be explored in future research.
Notes
Conflict of interest
Sang Woo Lyu is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
Author contributions
Conceptualization: SWL. Data curation: EJH, SWL. Formal analysis: EJH, SWL, WSL. Funding acquisition: SWL. Methodology: EJH. Project administration: WSL. Visualization: HNL, MKK. Writing–original draft: EJH. Writing–review & editing: SWL.
Supplementary material
Supplementary material can be found via https://doi.org/10.5653/cerm.2020.04266.
Sensitivity analysis using a random-effect model
Sensitivity analysis excluding unpublished trials
Risk of bias graph: a review of the authors’ judgments about each risk-of-bias item for each included study.
Risk of bias summary: a review of the authors’ judgements about each risk-of-bias item for each included study.
Meta-analysis of the clinical pregnancy rate (A) and live birth rate (B) according to the population type (previous implantation failure versus recurrent spontaneous abortion). M-H, Mantel-Haenszel; CI, confidence interval.