Outcomes of preimplantation genetic diagnosis using either zona drilling with acidified Tyrode's solution or partial zona dissection
Article information
Abstract
Objective
To review the outcomes of preimplantation genetic diagnosis (PGD) using zona drilling with acid Tyrode's solution (chemical zona pellucida drilling, chemical ZD) and those of partial zona dissection (PZD).
Methods
Clinical outcomes of seventy-one couples undergoing 85 PGD cycles from January 2005 to December 2010 were included. Blastocyst formation and the hatching rate, clinical pregnancy rate, ongoing pregnancy rate, implantation rate, and fetal gender ratio of the PZD and chemical ZD groups were compared.
Results
Application of PZD resulted in a significantly higher rate of clinical pregnancy (40.7% vs. 15.4%, p=0.022), ongoing pregnancy (35.6% vs. 11.5%, p=0.023), and implantation (18.1% vs. 5.7%, p=0.007) compared with chemical ZD. Among non-transferred embryos, the rate of blastocyst formation on day 5 (49.1% vs. 39.5%, p=0.016) and hatching on day 6 (47.2% vs. 26.5%, p<0.001) were also significantly higher in the PZD group.
Conclusion
The mechanical zona dissection method showed better outcomes than chemical ZD in terms of the blastocyst development and pregnancy rate. In this study, the fact that chemical ZD was conducted in different period from mechanical method should be considered in interpreting the result.
Introduction
Unlike conventional methods of prenatal diagnosis (i.e., amniocentesis, chorionic villi sampling [CVS]), preimplantation genetic diagnosis (PGD) enables us to detect any genetic abnormalities in an embryo before implantation. It has been successfully applied in couples with recurrent miscarriage due to parental chromosome abnormalities [1-3]. The success of the PGD procedure depends on the stage and grade of embryo, number of cells removed, and biopsy technique. Various techniques (i.e., mechanical dissection, chemical drilling, and laser ablation) for opening of the zona pellucida (ZP) have been developed [4-8]. However, not all of them have the same potential of success for PGD because the viability of embryo and/or blastomere may be affected by the biopsy procedure [9-12].
Chemical drilling methods include zona drilling with acid Tyrode's solution or zona thinning with a digestive enzyme like pronase. The major disadvantage of these techniques is the potential harmful effect on the embryo from the chemical agent. As a mechanical dissection method, partial zona dissection (PZD) is usually performed by cutting the ZP with a glass microneedle and generally requires experienced hands. Due to these limitations, according to a recent report of the ESHRE PGD Consortium, zona opening using a controlled laser beam is the predominant method at present [13]. Though laser ablation is convenient and requires a shorter working time, it may be difficult to use in several IVF centers due to its considerable cost [13,14]. Balaban et al. [15] compared four different techniques (PZD, zona drilling with acid Tyrode's solution or pronase, and the laser technique) for assisted hatching and obtained similar implantation and pregnancy rates. Embryo biopsy for PGD is a more complicated procedure than assisted hatching, and a key determinant for the success of PGD. However, comparative studies on the different embryo biopsy procedures including the resulting pregnancy rate are sparse.
In the present study, we retrospectively reviewed the results of two embryo biopsy techniques: PZD and zona drilling with acid Tyrode's solution. We evaluated the time needed to carry out the procedure, the success rate of retrieving a blastomere, and the rate of blastocyst formation and hatching for non-transferred embryos that were diagnosed as chromosomally abnormal. The clinical pregnancy, ongoing pregnancy, and implantation rates and the gender ratio were also compared.
Methods
A total of 85 IVF cycles with PGD from 71 couples in our clinic from January 2005 to December 2010 were included in this study. Most of the couples experienced two or more miscarriages; all of them had balanced translocations (male partner, 25; female partner, 42). Other indications of PGD included inversion of chromosome 6 (n=1), addition 8 (n=1), deletion 3 (n=1), and Klinefelter syndrome of the male partner (n=1).
1. IVF procedure
Pituitary down-regulation with buserelin (Suprefact, 0.6 mg/day; Sanofi-Aventis Deutschland GmbH, Hoechst, Germany) followed by controlled ovarian stimulation with recombinant follicle-stimulating hormone (Gonal-F, 150 IU/day; Serono, Geneva, Switzerland) and human menopausal gonadotropin (Menogon, 150-300 IU/day; Ferring, Malmo, Sweden) were performed as described elsewhere. When adequate follicular growth was demonstrated (more than two follicles reached 18 mm in diameter), hCG (Pregnyl, Organon, Oss, the Netherlands) was injected. After 35 to 36 hours, follicular aspiration was performed under the guidance of transvaginal ultrasound.
Sperm preparation was performed with centrifugation (1,400 rpm for 20 minutes) in discontinuous gradients (40%, 80%) of PureCeption (SAGE, Trumbull, CT, USA) and followed by the swim-up technique. The retrieved oocytes were cultured in Quinn's fertilization media (SAGE) and fertilized by ICSI.
Eighteen hours after sperm injection, normally fertilized oocytes were transferred to Quinn's cleavage media (SAGE). On the morning of day 2, the embryos were graded and transferred to the new Quinn's cleavage media and cultured until day 3. Good quality embryos were defined by the presence of 6 to 8 equal-sized cells with a fragmentation proportion below 25%.
2. Embryo biopsy
On the morning of day 3 after oocyte retrieval, embryos at the four- to eight-cell stage underwent blastomere biopsy. Zona drilling with acid Tyrode's solution for blastomere biopsy was used from January 2005 to December 2006. In this method, each embryo was individually placed in a 5 µL drop of phosphate buffered saline (PBS) without Ca2+ or Mg2+ (Gibco, Rockville, MD, USA) under mineral oil in a dish at 37℃. The embryo was held with a 30° angle holding pipette (MD plus, Seoul, Korea) and a small hole in the ZP was created by careful application of a small stream of acid Tyrode's solution (pH 2.4) with the use of a drilling pipette (inner diameter of the opening, 5-6 µm; MD plus). The acid solution was sucked back immediately once the ZP was drilled. Then the blastomere was aspirated with a biopsy pipette (MD plus) with an outer diameter of 50 µm and an inner diameter of 35 µm.
Modified PZD for blastomere biopsy was performed from January 2007 to December 2010. The small area of ZP close to the blastomere was selected and dissected with a PZD pipette (PZD pipette, Microtech, Brno, Czech Republic). It was an essential step to visualize the blastomere nucleus before ZP dissection and blastomere aspiration. A slit was made by rubbing the PZD pipette against the holding pipette with a sawing motion at the 12 o'clock position. The length of the slit was dependent on the size of each blastomere. The embryo was immobilized by holding the pipette and squeezed with a biopsy pipette until one selected blastomere was extruded. To aspirate the extruded blastomere entirely, the embryo was rotated until the extruded blastomere was positioned at 3 o'clock. The blastomere was then aspirated with a biopsy pipette (Microtech). Our method (aspiration after squeezing the embryo) was different from conventional PZD biopsy in which the blastomere was directly aspirated after zona dissection without squeezing.
When the biopsied blastomere had no nucleus or was lysed, another blastomere was obtained in both methods. Such a case was regarded as a "two-cell biopsy." Each biopsy procedure was performed by the same technician and observed by a second person on a monitor. For each blastomere biopsy, the presence of the nucleus and the operating time were recorded. The two-cell biopsy rate was defined as the percentage of blastocysts with two-cell biopsy among all of the blastocysts. The rate of successful retrieval of an intact blastomere was defined as the proportion of intact blastomeres among all of the biopsied blastomeres in each group. The operation time was defined as the time taken from transferring the embryo from PBS for micromanipulation to the culture drop after biopsy. All manipulation procedures were performed on heated stages.
The biopsied embryos were cultured in Quinn's blastocyst media (SAGE) until genetic diagnosis results were obtained and the biopsied blastomere was fixed individually. The blastomere was analyzed by FISH and only chromosomally competent embryos were transferred to the uterus on day 4. Biochemical pregnancy was confirmed by the presence of a positive serum level of β-hCG on day 9 after embryo transfer. Clinical pregnancy was defined as when fetal heartbeat was detected by ultrasonography. Ongoing pregnancy was determined after 24 weeks of pregnancy. The implantation rate was defined as the number of gestational sacs with a fetal heartbeat divided by the total number of embryos transferred. In all cases of pregnancy, chorionic villi samplings (CVS) were performed during 10 to 12 weeks and karyotypes were analyzed. After embryo transfer, chromosomally abnormal or unknown (non-transferrable) embryos were cultured until day 6 and development of each embryo was assessed. The rate of blastocyst formation on day 5 and hatching on day 6 were recorded.
3. Fixation of the retrieved blastomere
Each blastomere was placed in 0.075 M KCl for 1 minute and then washed with PBS solution (Gibco). The blastomere was moved to a degreased slide and 0.1% Tween 20/0.001 N HCl was added. After the cytoplasm was entirely removed, the slide was dried. After gentle dropping of Carnoy fixative (methanol:acetic=3:1) on it, the slide was scored under a phase-contrast microscope to locate the nucleus spreads. The slides were dehydrated in a series of 70%, 85%, and 100% ethanol for 1 minute each.
4. Fluorescence in situ hybridization
For hybridization, the blastomere DNA fixed on the slide was immersed and denatured in a 74±1℃ bath of 70% formamide in 2×saline-sodium citrate buffer (2×SSC) for 5 minutes. The nucleic acid probes were denatured with the same method. The slide was filled with the denatured probes, covered with a coverslip, and sealed with rubber cement. Then the slide was placed in an incubator at 37℃ overnight.
After hybridization, excess hybridization solution was washed out with 50% formamide in 1×SSC for 1 minute and then in 1×SSC for 1 minute at room temperature. The slides were counterstained with 4, 6-diamino-2-phenylindole (DAPI, Vysis, Des Plaines, IL, USA) and the signal was judged using two Olympus filters of red and green signals under a fluorescence microscope (Olympus BX50, Olympus Optical Co., Shinjuku, Japan). The criteria used to judge the signals were based on those described by Verlinsky and Kuliev [16]. Briefly, when the distance of two hybridization signals was at least two signal diameters, they were considered to be two separate signals. The others were considered split signals.
5. Statistical analysis
All variables were analyzed by the chi-squared and Student's t-tests to compare the clinical characteristics and outcomes of the two groups. A p-value less than 0.05 was considered significant. The statistical software package SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA) was used.
Results
A total of 71 couples were included in this study. PZD was performed in 59 cycles from 52 couples and chemical zona drilling in 26 cycles from 19 couples (Table 1). The success rate of single cell analysis was 87.5% (483/552) in the PZD group and 85.4% (276/323) in the chemical ZD group. The clinical and IVF cycle characteristics, such as the maternal age, number of retrieved oocytes, oocyte maturation rate, fertilization rate, number of transferred embryos, and rate of good quality embryos at the time of biopsy and transfer did not differ between the two groups (Table 2). A higher number of two-cell biopsies was observed in the PZD group. Technical factors such as the mean time for each biopsy procedure and the success rate of intact blastomere retrieval were not significantly different between the two groups.

Indications for preimplantation genetic diagnosis according to the biopsy method
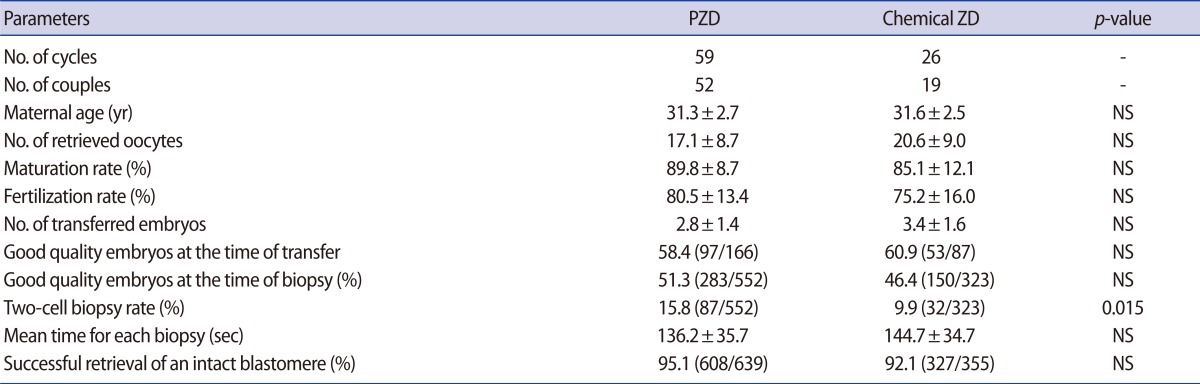
Clinical and ICSI characteristics according to the biopsy method
The clinical pregnancy, ongoing pregnancy, and implantation rate were significantly higher in the PZD group (Table 3). There were no cases of misdiagnosis since all of the karyotyping results from the CVS were found to be consistent with the PGD results. Fetal gender was identified in CVS and the gender ratio (XY/XX) was similar between the two groups (Table 3). The result of non-transferred embryo development according to biopsy method is shown Figure 1. The blastocyst formation rate on day 5 and hatching rate on day 6 were significantly higher in the PZD group.

Implantation, clinical pregnancy, and ongoing pregnancy rates and the fetal sex ratio in both groups
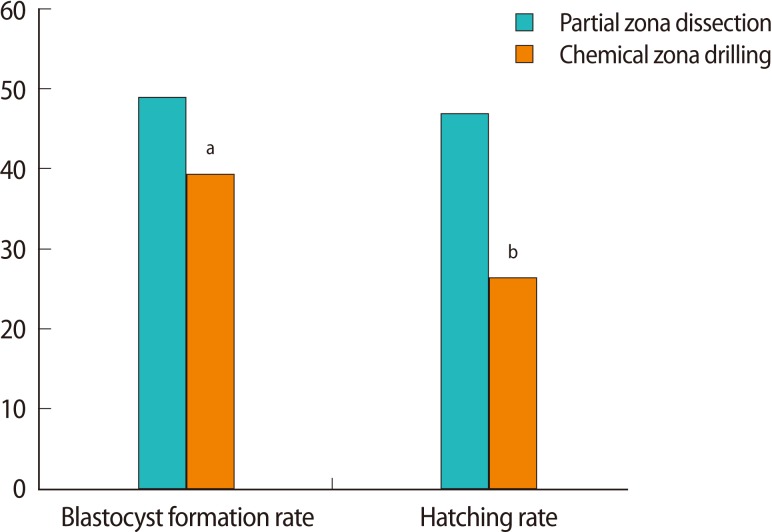
Rates of blastocyst formation and hatching in non-transferred embryos. ap<0.05, bp<0.01.
Discussion
Our study suggests that the mechanical method (PZD) for human blastomere biopsy may be more efficient than the chemical method (zona drilling with acid Tyrode's solution). The improved result of the PZD method might be due to the avoidance of the potential harmful effect of acid Tyrode's solution [17]. This results suggest that acid Tyrode's solution may impair embryo viability and further development after transfer [13]. In spite of a lower number of two-cell biopsies, the chemical zona drilling method showed a worse outcome than PZD. Because a higher number of biopsied blastomeres is known to be associated with a lower survival rate of blastocysts, this finding could reinforce the superiority of the PZD method in blastomere biopsy [18].
There are 7 cycles from the same couples in both the AT and PZD group, and this could have affected the result of this study. It is unclear whether these couples had to take more cycles because one of these methods is a less efficient method or the lower pregnancy rate was related to their lower fertility. Future controlled prospective studies will clarify this.
Considering the difference in the periods in which both methods were applied, there is a possibility that the superior results of PZD could be due to other factors, such as a better culture environment or more experienced hands of the technician. However, these effects would be minimized because there were no objective changes in the culture environment (the number of incubators, type of media, culture room conditions, and so on) in this period and the technician had already had several years of PGD experience at the beginning of this study. Moreover, since there was no significant difference in the fertilization rate after ICSI in both groups, the improved outcome of the PZD group is likely to be at least partially explained by the embryo biopsy method itself.
In grading blastocysts, because male embryos reach advanced stages faster than female embryos, it is postulated that more male embryos might have been selected for transfer [18]. But the similar gender ratio between the two groups in this study supports the recent research of Eaton et al. [19] who found that the chance of development to blastocyst and rate of euploidy is not sex-dependent. The developmental ability of chromosomally abnormal human embryos has been known to differ according to the type of chromosomal abnormality [19-21]. A recent report revealed that embryos with unbalanced translocations were able to reach the blastocyst stage [22]. However, it is unclear whether differing chromosomal anomaly corresponds to a specific arresting stage. Since the rate of reciprocal translocations and Robertsonian translocations were similar in the two groups (Table 1), the potential effect of different chromosomal abnormalities might have been minimized in our results.
Although there was no statistical significance between the two groups, the shorter operating time of the PZD group (136.2±35.7 vs. 144.7±34.7) might have reduced the extent of embryonic exposure to suboptimal conditions outside the incubator. In the chemical ZD group, it took additional time to fill the drilling pipette with acid Tyrode's solution and control the amount of the solution in ZP drilling followed by several washing procedures to remove any residual acid.
Compared to the result of other reports in which PZD and zona drilling with acid Tyrode's solution were used, both methods needed a relatively shorter time in our study [23]. With regard to the percentage of viable blastomeres, a relatively higher number of viable blastomeres were successfully obtained (about 95.1%) in the PZD group than the chemical ZD group. Considering that intact DNA of the biopsied blastomere is critical in the PGD procedure, this result may underline the superiority of the PZD method. In recent recommendations, mechanical zona drilling is considered 'acceptable' for first polar body biopsy when performed before fertilization, but acidic Tyrode's or laser are considered 'not recommended' as they may adversely affect the spindle [24-26]. Therefore, it should be determined whether the use of acidic solution has a detrimental effect on the mitotic spindle of blastomeres in metaphase [27].
The PZD method developed by Malter and Cohen had been used as the fertilization method until ICSI was developed [28]. A fine microneedle is pierced through the zona, in at the one-o'clock position and out again at the eleven o'clock position to create a relatively small opening. This method helps the oocyte be inseminated by creating an opening in the zona through which the spermatozoa can swim. In the embryo biopsy, a relatively larger opening was made compared to the assisted fertilization method.
Several modified mechanical dissection methods have been reported: piezo-micromanipulator, three-dimensional (3D) PZD, and controlled zona dissection (CZD). Reduction and breaching of the ZP are achieved mechanically by the vibratory motion of a needle produced by a piezo-electric pulse in the piezo-micromanipulator method [29]. A cross-shaped opening by the delicate use of a microneedle is made in the 3D-PZD [30]. The long distance of the zona dissection is made using a modified holding pipette in CZD [31]. Compared to these three methods, our modified PZD method might be simpler. Furthermore, in our method, the zona opening and blastomere aspiration after squeezing requires no additional instruments and could result in a more intact blastomere than in conventional PZD, which involves direct aspiration [32].
Zona drilling using a laser is currently proposed as a technically easier method compared to mechanical and chemical means. Although there are reports that laser drilling does not impair embryonic development to the blastocyst stage and implantation [13,14,33,34], it has been postulated to pose potential harm to embryos in previous studies [31,35,36]. Furthermore, a laser is not cost-effective for IVF laboratories where PGD procedures are not performed frequently. Considering the safety issue and relatively high cost, our modified PZD method could be a good alternative.
In summary, the PZD method showed better clinical outcomes in our study although there are several limitations given its retrospective design. Our PZD method could be a safe and cost-effective choice in many IVF laboratories that plan to set up PGD. To confirm which one of these blastomere biopsy methods is superior, further prospective studies would be needed.
Notes
No potential conflict of interest relevant to this article was reported.