Predictive value of sperm motility characteristics assessed by computer-assisted sperm analysis in intrauterine insemination with superovulation in couples with unexplained infertility
Article information
Abstract
Objective
To determine whether characteristics of sperm motility obtained by computer-assisted sperm analysis (CASA) could predict pregnancy after intrauterine insemination (IUI) in couples with unexplained infertility.
Methods
Three hundred eighty-three cycles of intrauterine insemination with superovulation were retrospectively analyzed. Semen analysis was performed with CASA before and after swim-up and the parameters were compared between pregnant and non-pregnant women.
Results
The pregnancy rate per cycle was 14.1%. Pregnant and non-pregnant women were comparable in terms of age, infertility duration, the number of dominant follicles. While sperm concentration, motility, and parameters such as average path velocity (VAP) and percentage rapid (RAPID) before semen preparation were significantly different between the pregnancy and non-pregnancy groups, there were no differences in sperm parameters when comparing the two groups after preparation. Using a receiver operating characteristic curve to measure sensitivity and specificity, the optimal threshold value for the predictors of pregnancy was revealed to be a concentration of ≥111×106/mL, a motility of ≥51.4%, and RAPID ≥30.1% before preparation for IUI.
Conclusion
Sperm parameters including concentration, motility, and RAPID before sperm preparation could have predictive value for pregnancy outcome after intrauterine insemination with superovulation in couples with unexplained infertility, and would be helpful when counseling patients before they make the decision to proceed with IVF/ICSI-ET.
Introduction
Although assisted reproductive technologies (ARTs) including in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) have been developed, intrauterine insemination (IUI) still remains a reliable method that can be applied to many infertile couples. Compared to IVF or ICSI, IUI is less invasive and associated with lower costs and a low incidence of complications, making it a relatively cost-effective treatment for many forms of infertility [1]. Indications for IUI have included mild male factor infertility (oligozoospermia, asthenozoospermia, pyospermia), cervical factor infertility, and cases of unexplained infertility.
In cases of unexplained infertility, the pregnancy rate with IUI has been reported to be 9-20% [2-5]. Moreover, a meta-analysis revealed that the live birth rate of IUI increased twofold when it was undergone with ovarian stimulation rather than the natural cycle [6]. The success rates of IUI with superovulation depend on the woman's age, duration of infertility, sperm quality, and tubal patency on either side [3,7]. Among sperm parameters, total motile sperm count and morphology are known to be closely associated with the success of IUI [2,8-10].
Standard semen quality assessment describes the volume, viscosity, concentration, normal and abnormal morphology, and motility of spermatozoa when conducted according to guidelines by the World Health Organization (WHO) [11]. However, it is a rather subjective method which has been associated with large inter-laboratory variation in estimating the respective percentages of progressive and non-progressive motile and immotile spermatozoa, which makes it difficult to predict fertility [12,13]. In an attempt to make assessments of sperm movements more objective and detailed, tools for computer-assisted sperm analysis (CASA) have been developed. CASA is an automated method used to visualize sperm that can assess several specific motility parameters describing the movements of spermatozoa. Several studies have addressed CASA parameters as predictors of male fertility. Larsen et al. [14] reported that CASA parameters were useful in predicting the possibility of natural pregnancy in the general male population. In studies of male infertility, some CASA parameters were reported to be useful in predicting pregnancy after IUI with partner or donor sperm [15-18], and in the assessment of sperm fertilizing ability in IVF [19].
On the other hand, some studies have failed to show the association of CASA parameters with the success of IUI [20,21], and there have been few studies about its usefulness in predicting pregnancy after IUI in cases of unexplained infertility.
The aim of this study was to determine whether assessing characteristics of sperm motility using CASA could predict pregnancy after IUI with superovulation in couples with unexplained infertility.
Methods
1. Subjects
This is a retrospective case-control study that was performed in our infertility clinic between October 2006 and September 2008. Three hundred and eighty-three patients with unexplained infertility that underwent IUI with superovulation were included in this study. Patients were divided into two groups, the pregnant group and non-pregnant group.
The inclusion criteria were a follicular stimulating hormone (FSH) level no greater than 12 mIU/mL, at least unilateral tubal patency demonstrated in hysterosalpingogram, and semen analysis resulting in normal sperm counts, morphology, and motility according to the WHO classification. Exclusion criteria were a woman's age of more than 40 years, ovarian cyst detected in the ultrasound examination, uterine lesions such as submucosal leiomyoma, and a previous diagnosis of moderate to severe pelvic endometriosis.
Successful pregnancy after intrauterine insemination was confirmed by ultrasound as one or more visible gestational sacs in the uterine cavity.
2. Superovulation and intrauterine insemination
Superovulation was conducted with either 150 IU of intramuscularly injected uhMG (IVF-M; LG Life Science, Seoul, Korea) or 100 mg of oral clomiphene citrate (Clomifene; Young Poong Pharmaceutical, Incheon, Korea) for five days starting on day 3 of the menstrual cycle, followed by daily injection of 150 IU of hMG. When more than two dominant follicles reached a diameter of 17 mm or the urinary specimen showed positive results for LH surge, 5,000 IU of hCG (Pregnyl; Organon, Oss, the Netherlands) was injected intramuscularly, and after 24 to 36 hours, IUI was performed only once.
Semen was collected from subjects via ejaculation after at least 48 hours of abstinence. The semen was then analyzed after at least 30 minutes of liquefaction. For semen analysis, 10 µL of semen was analyzed by computer assisted sperm analysis (CASA; Sperm Analysis Imaging System [SAIS] ver. 10.1, Medical Supply, Wonju, Korea), and concentration, sperm motility, total motile sperm count, hyperactivity percent (HYP), curvilinear velocity (VCL), straight line velocity (VSL), average path velocity (VAP) , linearity (LIN), straightness (STR), beat cross frequency (BCF), and amplitude of lateral head displacement (ALH), percentage rapid (RAPID) were reported. Semen preparation was performed using the conventional swim-up method, and the same parameters were reanalyzed via a computerized process.
3. Statistical analysis
Statistical analysis was carried out with the SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA). Calculations of statistical differences between the groups were carried out by a Student's t-test or a chi-square test. Receiver operating characteristic (ROC) curves were constructed for the calculation of the clinically acceptable cut-off value of each individual parameter in predicting pregnancy by IUI. A p-value of <0.05 was defined as representing a significant difference.
Results
A total of 383 cycles of intrauterine insemination with superovulation were conducted. There were 54 cases of successful intrauterine pregnancy and the pregnancy rate was estimated to be 14.1%. There were no significant differences between the pregnant group and the non-pregnant group in terms of female age, duration of infertility, basal hormone levels, number of dominant follicles, or endometrial thickness at the time of hCG administration (Table 1).
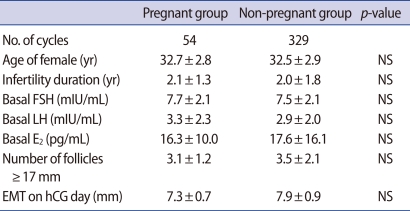
Patient characteristics of pregnancy and non-pregnancy groups
Statistically significant differences were found in some variables associated with semen analysis before swim-up: sperm concentration (152.9±13.7×106/mL vs. 118.8±4.3×106/mL in the pregnant and non-pregnant group, respectively; p=0.021); motility (56.8±1.8% vs. 51.2±0.9%; p=0.007); VAP (40.8±1.05 µm/sec vs. 38.4±0.4 µm/sec; p=0.033); and RAPID (28.1±2.16% vs. 24.5±0.87%; p=0.022). VCL (67.2±1.85 µm/sec vs. 63.3±0.74 µm/sec; p=0.050) and VSL (32.8±1.01 µm/sec vs. 30.7±0.37 µm/sec; p=0.050), parameters of sperm motility, showed some degree of difference that was not statistically significant. Differences in LIN, STR, BCF, and ALH were not statistically significant. After swim-up, semen analysis parameters were not significantly different between the two groups (Table 2).
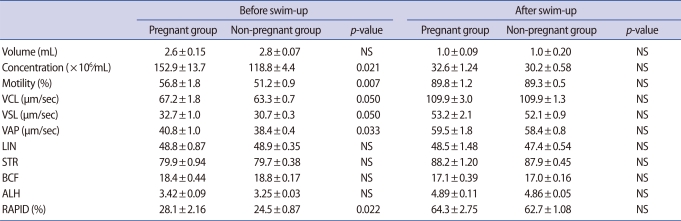
Semen parameters before and after swim-up
According to the ROC curve, RAPID, motility, and concentration parameters in the unprocessed semen were predictive of pregnancy and the cut-off values were 30.1% for RAPID, 51.4% for motility, and 111×106/mL for concentration. Further analysis was performed according to the number of parameters that were consistent with these criteria. The pregnancy rate per cycle was 6.7% (7/104) if no criteria were met, 11.4% (13/114) for one criterion, 15.7% (11/70) for two criteria, and 24.2% (23/95) if all three criteria were met (Tables 3, 4, Figure 1).
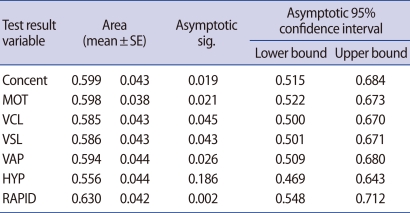
Comparison of CASA parameters as predictors of pregnancy using ROC curves
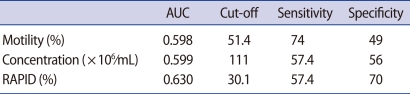
ROC curve analysis: AUC and cut-off with best sensitivity and specificity combination
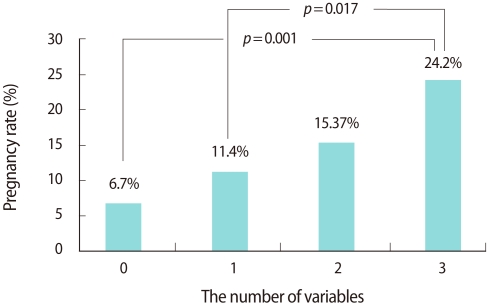
Association between pregnancy rate and number of variables exceeding the threshold for the three independent predictive parameters.
Discussion
Intrauterine insemination with or without superovulation is usually the first-line treatment choice for patients with unexplained infertility who failed to conceive by conventional ovulation induction with timed coitus. Although the IUI procedure is less invasive and less expensive than IVF or ICSI, both infertile couples and doctors bear a psychological burden because of the relatively low success rate per cycle, leading to a repetition of the procedure and a risk of higher-order multiple pregnancy associated with superovulation [1,2,4,5].
Many investigators have attempted to determine the optimal predictor of success to help counsel patients before they make the decision to proceed with IVF/ICSI-ET. It is known that female age, duration of infertility, tubal patency, the number of induced follicles, the insemination technique, timing, and several semen parameters may affect the outcome of the IUI procedure [3,7]. Among semen parameters, sperm motility is believed to be one of the most important characteristics correlated with fertility [22,23].
Prospective studies have shown that the conventional semen profile of the WHO is unable to discriminate between fertile and infertile men, especially in idiopathic infertility [22,24-26]. Accordingly, additional functional tests, such as the zona-free hamster egg penetration test [27] and evaluation of acrosome reaction combined with assessments of cell viability [28], have been suggested to provide more information on the fertilizing potential of human spermatozoa in addition their number or appearance. However, many of the assays involved are technically complex.
CASA is an automated method that can measure several specific motility parameters that describe the movements of spermatozoa with the advantage of providing more objective, reproducible, and detailed data on sperm motility. Many studies have indicated that the direct quantitative assessment of sperm movement by CASA reflects the fertilizing ability of human spermatozoa in vitro under conditions where the conventional semen profile is of limited diagnostic value. A prospective follow-up study reported that the concentration of motile spermatozoa, defined as spermatozoa with a VCL>25 µm/sec, was the most significant and independent CASA parameter in predicting the chance of natural conception in the general male population [14]. Barratt et al. [29] found the total number of spermatozoa and VAP to be predictors of pregnancy. Other parameters such as ALH, VSL, VCL, and LIN have also been reported to be correlated with fertility [28,30].
The relative influence of semen parameters on the likelihood of a successful outcome in IUI remains controversial. Shibahara et al. identified three semen parameters including normal morphology ≥15.5% before sperm separation, rapid motility >25.5%, and VCL>102.6 µm/sec after sperm preparation as predictors of pregnancy by IUI in male infertility, and reported that no pregnancy was acheived if none of these three parameters were satisfied [15]. Freour et al. [20] found that the concentration and proportion of progressive motile spermatozoa, defined as cells with VAP>25 µm/sec and VSL>100 µm/sec, were higher in the pregnancy group than in the failure group, while respective sperm motility parameters measured by CASA failed to predict pregnancy in IUI cycles conducted with donor sperm. They also reported that ALH improvement during the sperm preparation is necessary for pregnancy in an IUI with frozen donor semen and speculated that it could help in improving pregnancy rates in IUI with donor semen programs, as ALH evolution before and after preparation can be easily calculated [21].
In a retrospective analysis of the relationship between the CASA estimates and fertilization rates in IVF-ET cycles, two parameters, including VCL and rapid, provide reliable estimations of the fertilizing ability of human sperm [19].
Most of the studies on CASA parameters and fertility outcome in IUI have been conducted in couples with male infertility, whereas few studies were conducted in couples with unexplained infertility. In this study, we assessed the sperm motility parameters by CASA in 383 IUI cycles with superovulation indicated in couples with unexplained infertility. Specific CASA parameters such as VAP, RAPID, VSL, VCL, as well as sperm concentration and motility were significantly different between the pregnant group and the non-pregnant group. We also found that the combination of parameters such as RAPID ≥30.1%, motility ≥51.4%, and concentration ≥111×106/mL before sperm preparation could be useful in predicting pregnancy in IUI. For instance, the pregnancy rate was highest if all three parameters were satisfied, while it was lowest if no parameters were satisfied.
Many studies reported that the improvement of sperm motility parameters during the preparation process or their value after preparation were correlated with their pregnancy outcome of IUI [15-21], whereas we did not find any difference between CASA parameters after sperm preparation according to cycle outcome. This may have been due to our use of fresh semen of normal values by WHO criteria, in contrast to previous studies that utilized semen with male factor infertility or frozen-thawed donor sperm.
In general, one of the most important movements associated with sperm fertilizing ability is known to be hyperactivated motility [31,32]. Hyperactivation is characterized by the development of high velocity, large amplitude, asymmetrical flagellar waves, and is thought to facilitate the detachment of spermatozoa from the oviductal epithelium and penetration of the matrix of the cumulus oophorus and the zona pellucida [32]. CASA has been used to detect hyperactivation, as it generates a characteristic non-progressive star-spin pattern of movement, and to identify the percentage of sperm in a sample that are hyperactivated. As for hyperactivation, we did not find any difference between the pregnant and the non-pregnant groups. Also, there was no difference in the pregnancy rate according to hyperactivation. It can be postulated that hyperactivation occurred when the spermatozoa reached the oocyte vicinity and CASA could only be of limited value to the assessment of hyperactivation in vitro before the IUI procedure. Unfortunately, factors triggering hyperactivation in vivo are poorly understood, and it has been suggested that the trigger may be hormones, ions, secretions of the oviductal epithelium, or a change in the pH of oviduct fluid or follicular fluid introduced into the oviduct by the oocyte-cumulus mass [33,34].
In conclusion, concentration and motility assessment of semen by CASA is a fairly useful method for predicting pregnancy outcome after IUI with superovulation, which could be helpful in planning strategies for the further treatment of unexplained infertile couples by proceeding with IVF/ICSI-ET.
Notes
No potential conflict of interest relevant to this article was reported.