Introduction
Complete androgen insensitivity syndrome (CAIS), or testicular feminization, is a rare X-linked recessive disease characterized by variable defects in virilization of individuals with male karyotype (46,XY) and an absence of sex chromatin. CAIS is caused by mutations in the androgen receptor gene, resulting in impaired embryonic sex differentiation and producing a female external phenotype.
Most patients with CAIS are diagnosed at puberty with primary amenorrhea. Although their risk of malignancy is extremely low, malignant transformation of dysgenetic male gonads (undescended testes) has shown a significant association with aging. We describe here a 58-year-old patient, never previously diagnosed with CAIS, who presented with a large, late stage malignant seminoma as the primary presentation of CAIS.
Case report
A 58-year-old woman was referred from a primary clinical to the Department of General Surgery at Asan Medical Center (Seoul, Korea) for an inguinal hernia. She had noticed reducible swellings on both inguinal areas for 10 years but did nothing until the swellings became problematic. These swellings had increased 7 months earlier, accompanied by pain. Ultrasound examination showed a well-defined cyst in the right inguinal area, and a mass with cystic and solid portions in the left inguinal area. Computed tomography showed a 7.4 cm round homogeneously enhanced mass in the left inguinal canal with an enlarged lymph node in the left para-aortic area (Figure 1).
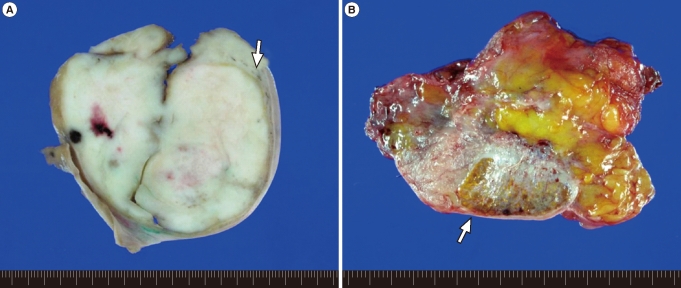
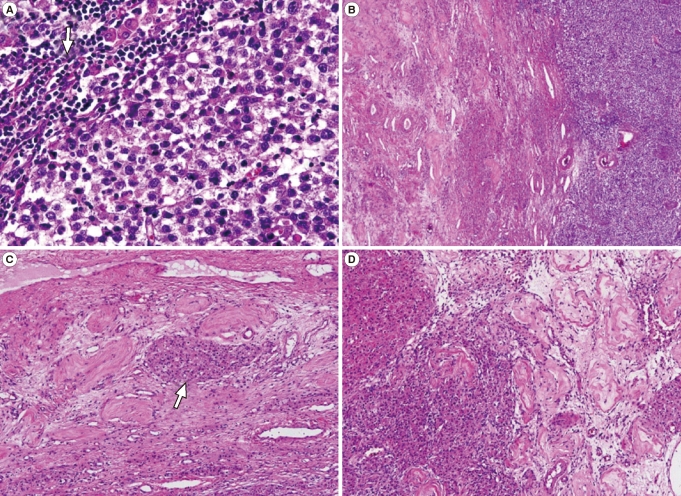
The mass excised from the left inguinal area was well-defined and firm, measuring 7├Ś7├Ś6 cm in size. The cut surface was homogenously creamy white and vaguely lobulated with focal hemorrhage (Figure 2A). The mass in the right inguinal canal was heterogeneously golden yellow to pinkish gray and encapsulated (Figure 2B). Microscopically, the mass of left inguinal area consisted of large uniform cells growing in broad sheet divided by thin septa which infiltrated by lymphocytes. The nuclei of the tumor cells were centrally located and round to polygonal with finely granular chromatin and prominent nucleoli. The cytoplasm was eosinophilic to clear and had distinct cell border (Figure 3A). These features were consistent with seminoma of classic type. Adjacent to the mass was soft tissue composed of atrophic hyalinized seminiferous tubules and interspersed Leydig cell nests in between, compatible with testicular tissue (Figure 3B, 3C). The mass from right inguinal canal also had testicular tissue with atrophic hyalinized seminiferous tubules, but the leydig cell nests were larger and more abundant, consistent with leydig cell hyperplasia (Figure 3D). This mass was removed surgically, as was the reducible mass in the right inguinal canal, followed by herniorrhaphy.
Postoperatively, the surgeon in charge requested a detailed examination of this patient by a gynecologist for further evaluation and treatment. The patient was amenorrheic for her entire life, is unmarried, and a virgin. She was 170 cm in height and weighed 80 kg. Physical examination showed that her breasts were normally developed, but her pubic hair and axillary hair were sparse. She had slightly enlarged external genitalia with a blindly-ending vagina about 2 cm long. Chromosomal analysis showed a 46,XY karyotype, but none of her previous gynecological examinations had diagnosed any distinct features. Her serum testosterone concentration was 0.25 ng/mL (normal male range, 2.6-15.9 ng/mL) and her estradiol concentration was 12.1 pg/mL (normal male range, 0-44 pg/mL). Based on these findings, the patient was diagnosed with AIS. Because computed tomography suggested metastasis along the left para-aortic lymph node, adjuvant radiotherapy and chemotherapy were recommended.
Discussion
CAIS, originally called complete testicular feminization, is a phenotype resulting from a defect in androgen receptor function and causes peripheral androgen resistance. Since the androgen receptor is encoded by a gene located on chromosome Xq11-12, CAIS is an X-linked recessive disease. It is characterized as a male karyotype with a normal female phenotype, such as female breast development, although there is little or no axillary and pubic hair. The external genitalia appear normal or slightly underdeveloped and the vagina is of varying length, but is usually shortened and with a blind ending. Internal genitalia, including the cervix and uterus, are absent except for undescended testes in the abdominal cavity or inguinal or labia majora along the normal course of testicular descent.
These patients have a plasma testosterone concentration within the normal range in males. However, some patients have elevated plasma testosterone due to increased stimulation by luteinizing hormone. In contrast, our patient had a decreased testosterone level, probably due to her completely atrophied testes.
The prevalence of CAIS in the general population ranges between 1 in 20,000 and 1 in 60,000 in females. It is the third most frequent cause of primary amenorrhea and is the most common form of male pseudohermaphroditism.
Fortunately, CAIS is usually diagnosed at puberty after an individual presents with primary amenorrhea or an inguinal hernia. A few retrospective studies have estimated that 0.8% to 2.4% of girls with inguinal hernias have CAIS [1]. Therefore, phenotypic female infants with an inguinal hernia should be fully evaluated. Lack of awareness of the association between inguinal hernias in girls and CAIS has often led to failure to make an early diagnosis, particularly in the past.
The risk of malignancy in patients with CAIS increases with age. For example, 3.6% of 25-year-old and 33% of 50-year-old AIS patients are likely to have tumors [2]. Tumors in these patients are due to undescended testes, accounting for 10% of patients with testicular tumors [3]. The two most frequent types of testicular tumors associated with AIS are Sertoli cell and germ cell tumors. Several long-term follow-up studies have shown that the timing of gonadectomy in women with CAIS can be delayed until sexual maturation is complete, because patients with CAIS have a normal pubertal growth spurt and feminize at the time of expected puberty, and usually do not develop malignant tumors until puberty [4]. Therefore, prophylactic gonadectomy after puberty is recommended [5]. Routine ultrasound examination is recommended to monitor potential malignant changes in the gonads of these patients.
We describe here an older woman with advanced seminoma who presented with a bilateral inguinal hernia and was first diagnosed with CAIS. The diagnosis of CAIS was delayed in this patient, and she failed to receive appropriate care, resulting in the development of a seminoma and its progression to an advanced stage.