The impact of two doses of coenzyme Q10 on semen parameters and antioxidant status in men with idiopathic oligoasthenoteratozoospermia
Article information

Abstract
Objective
Oxidative stress contributes to male infertility, and antioxidants have been recommended for treating idiopathic oligoasthenoteratozoospermia (OAT). There is, however, a lack of agreement on the type, dosing, and use of individual antioxidants or combinations thereof. The purpose of this study was to compare the effects of two doses of coenzyme Q10 (CoQ10) on semen parameters and antioxidant status in men with idiopathic OAT.
Methods
In this prospective study, patients with idiopathic OAT received 200 mg/day (n = 35) or 400 mg/day (n = 30) of CoQ10 orally for 3 months. All patients underwent semen analysis according to the fifth editions of the World Health Organization criteria. Total antioxidant capacity (TAC), catalase (CAT) activity, and superoxide dismutase (SOD) activity were measured both before and after treatment.
Results
Treatment with CoQ10 (200 mg/day or 400 mg/day) resulted in a significant increase in sperm concentration from baseline (8.22 ± 6.88 to 12.53 ± 8.11 million/mL, p= 0.019; 7.58 ± 5.41 to 12.33 ± 6.1 million/mL, p= 0.002, respectively), progressive motility (16.54% ±9.26% to 22.58% ±10.15%, p=0.011; 14.22% ±12.85% to 26.1% ±14.52%, p= 0.001, respectively), and total motility (25.68% ± 6.41% to 29.96% ± 8.09%, p= 0.016; 23.46% ± 12.59% to 34.82% ± 14.17%, p= 0.001, respectively). CoQ10 therapy also increased TAC (p= 0.009, p= 0.001, respectively), SOD activity (p= 0.004, p= 0.001, respectively), and CAT activity (p= 0.039, p= 0.024, respectively). Furthermore, antioxidant measures correlated significantly with seminal fluid parameters (r = 0.36–0.76).
Conclusion
CoQ10 supplementation improved semen parameters and antioxidant status in men with idiopathic OAT, with a greater improvement shown in men who took 400 mg/day than in those who took 200 mg/day.
Introduction
The prevalence of infertility has increased significantly in recent decades, and it is currently estimated to affect approximately 15% of the population worldwide [1]. Male infertility has been linked to many factors, including varicocele, infections, undescended testis, and autoimmune, endocrine, genetic, and environmental factors [2]. However, no underlying cause for infertility is identified in 30%–40% of patients; such cases are termed idiopathic male infertility (IMI). Potential mechanisms underlying IMI include genetic, biochemical, hormonal, and environmental factors [3].
Oxidative stress (OS) has been proposed as a mechanism underlying IMI. OS is defined as a disruption of the prooxidant-antioxidant balance that leads to DNA damage, peroxidation of plasma membrane lipids, and protein oxidation [4]. OS occurs when reactive oxygen species (ROS) disrupt the equilibrium of reduction and oxidation. ROS are highly reactive molecules produced during normal cellular metabolism and physiology, formed due to the incomplete reduction of oxygen [5]. In seminal plasma, ROS play a fundamental physiologic role in several sperm functions, such as the development, maturation, and capacitation of spermatozoa, as well as the acrosome reaction and fertilization [6]. Sperm cells and leukocytes are the main sources of ROS in seminal plasma. Although adequate amounts of ROS are crucial for normal sperm function, excess levels trigger OS and negatively affect reproductive outcomes [4,7]. ROS affect sperm motility by altering axonemal protein phosphorylation and sperm membrane fluidity. Furthermore, ROS may induce sperm DNA damage, including DNA deletion, cross-linking, and chromosome rearrangement, leading to impaired fertilization, abnormal embryonic development, and possibly, congenital foetal defects.
Spermatozoa have a limited intrinsic antioxidant capacity and DNA repair system [8]. However, semen contains several endogenous and exogenous antioxidant molecules that allow maintenance of the balance between reduction and oxidation, including catalase (CAT), superoxide dismutase (SOD), glutathione peroxidase, vitamin C, vitamin E, coenzyme Q10 (CoQ10), carnitine, selenium, zinc, copper, and carotenoids [9,10]. Nevertheless, in men with IMI, poor semen quality is associated with decreased antioxidant capacity [11]. Both increased ROS production and reduced seminal plasma antioxidant capacity have been reported in infertile men [12].
CoQ10 is a lipid-soluble compound synthesized de novo, which may be found in a reduced (ubiquinol) or oxidized (ubiquinone) form [1]. Endogenous CoQ10 levels are closely related to overall oxidative activity, as it plays a role in mitochondrial bioenergetics as part of the mitochondrial respiratory chain [13]. CoQ10 also modulates gene expression, cell signalling, transport, and metabolism. Moreover, the reduced form acts as an electron acceptor in plasma and subcellular fractions [14].
Studies have demonstrated low levels of CoQ10 in infertile men [1,3]. Further, CoQ10 supplementation was associated with improvement of 1 or more seminal fluid parameters [15]. A placebo-controlled study found that in infertile men with oligoasthenoteratozoospermia (OAT), CoQ10 treatment improved semen parameters and antioxidant status [16]. A meta-analysis by Lafuente et al. [3] reported improvements in sperm concentration and motility, as well as an increase in seminal CoQ10 levels. Several studies have shown beneficial effects of antioxidant treatment in infertile men [17-19]. However, there is no consensus on the type, dosing, patient selection, and the use of individual or combination therapy [20]. In this context, the objective of this study was to evaluate the effect of oral CoQ10 at doses of 200 mg/day or 400 mg/day for 3 months on sperm parameters and seminal plasma antioxidant status in infertile men with idiopathic OAT.
Methods
1. Patients
Out of 70 patients initially selected for the study, 65 patients (mean age, 27.24±7.81 years) with idiopathic OAT were recruited at the Fertility Clinic, Babil Governorate, Iraq from June to November 2018 and enrolled in the study (five patients did not complete the study). All patients underwent a medical assessment including a history, physical examination, and laboratory and radiological investigations. The study was conducted as a prospective randomized clinical trial with 3 months of follow-up. The selected patients who fulfilled the selection criteria were randomly assigned to two treatment groups. Group 1 (n=35) received 200 mg (single dose) of oral CoQ10 and group 2 (n=30) received 400 mg (single dose) of oral CoQ10 (in the reduced form ubiquinol; America Medic and Science, Woodinville, WA, USA) daily for 3 months. The first group served as active control. We chose CoQ10 doses analysed in previous studies [1,21]. Semen analysis was performed, and total antioxidant capacity (TAC), CAT, and SOD activity were measured in seminal plasma samples and compared before and after therapy.
2. Eligibility criteria
The inclusion criteria comprised a history of infertility lasting for at least 12 months despite regular unprotected intercourse. OAT was diagnosed by semen analysis results showing abnormal sperm concentration (<15 million/mL), progressive motility (<32%), and total motility (<40%) as defined by the fifth edition of the World Health Organization (WHO) criteria for semen analysis [22] and abnormal morphology (<30% normal morphology) as defined by the fourth edition of the WHO criteria [23]. The exclusion criteria comprised azoospermia, varicocele, genital tract infection, cryptorchidism, testicular trauma or scrotal surgery, endocrine disorders, systemic illness including hepatic and renal diseases, smoking, recent intake of antioxidants, and the presence of female factor infertility.
3. Semen analysis
Semen samples were obtained by masturbation after sexual abstinence for 2–3 days, collected in a sterile wide-mouth plastic container, kept at 37°C until liquefaction, and then analysed within 1 hour of production using the manual method according to fifth edition of the WHO criteria [22] and the fourth edition criteria [23] for sperm morphology. Semen volume, sperm concentration, motility, and morphology were measured. All semen analyses were performed by the same investigator for the sake of data consistency, and all patients underwent two semen analyses before and after therapy; the average values were used.
4. Seminal TAC
Semen samples were centrifuged at 3,000 rpm for 5 minutes, and the seminal plasma was aspirated and stored frozen for further biochemical analysis. TAC was measured by a colorimetric method using the total antioxidant capacity assay kit (#E-BC-K136; Elabscience, Houston, TX, USA). The test is based on the principle that antioxidants in the body can reduce Fe3+ to Fe2+ and that Fe2+ can form stable complexes with phenanthroline. The TAC was calculated by measuring the absorbance at 520 nm using a standard protocol.
5. Seminal SOD activity
SOD activity was determined by a colorimetric method as described by Magnani et al. [24]. The principle of this method is based on competition between pyrogallol autoxidation by superoxide anion and scavenging of this radical by SOD. The activity of SOD was calculated by measuring the absorbance at 420 nm using a standard protocol.
6. Seminal CAT activity
Seminal CAT activity was determined by a colorimetric method using the CAT assay kit (#E-BC-K031, Elabscience). The test is based on the principle that the process through which CAT decomposes H2O2 can be quickly stopped by ammonium molybdate. The residual H2O2 reacts with ammonium molybdate to generate a yellowish complex. CAT activity was calculated by measuring the absorbance of the yellowish complex at 405 nm using a standard protocol.
7. Statistical analysis
IBM SPSS ver. 24.0 (IBM Corp., Armonk, NY, USA) was used for all statistical analyses. The results were expressed as mean±standard deviation. The Kolmogorov-Smirnov test was used to assess the normality of the data. The paired t-test was used to compare mean values before and after treatment. The Pearson correlation coefficient (r) was used to evaluate correlations between seminal parameters and TAC, CAT, and SOD. The p-values less than 0.05 were considered to indicate statistical significance.
8. Human and animal rights
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. The study protocol was approved by local Ethical Committee at University of Sumer, Iraq and all participants provided informed consent for participation in the study NCT03850561 (https://clinicaltrials.gov/).
Results
A total of 65 patients were included in the study, with 35 patients in group 1 and 30 patients in group 2. The mean age was 26.23±7.22 and 29.45±8.61 years in groups 1 and 2, respectively (p=0.094), while the mean duration of infertility was 4.34±3.64 and 4.91±4.17 years in groups 1 and 2, respectively (p=0.54) (Table 1). Treatment with CoQ10 (200 mg or 400 mg per day) resulted in a significant increase in sperm concentration from baseline (8.22±6.88 to 12.53±8.11 million/mL, p=0.019; 7.58±5.41 to 12.33±6.1 million/mL, p=0.002, respectively), as well as improvements in progressive motility (16.54%±9.26% to 22.58%±10.15%, p=0.011; 14.22%±12.85% to 26.1%±14.52%, p=0.001, respectively), and total motility (25.68%±6.41% to 29.96% ±8.09%, p=0.016; 23.46%±12.59% to 34.82%±14.17%, p=0.001, respectively). These changes were greater in the group treated with 400 mg of CoQ10 (Table 1).
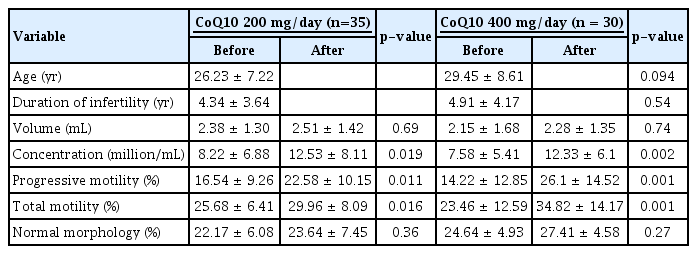
Patient characteristics and semen parameters before and after CoQ10 treatment (200 and 400 mg/day)
Likewise, treatment with CoQ10 (200 mg/day or 400 mg/day) resulted in significant increases in TAC (p=0.009, p=0.001, respectively), SOD activity (p=0.004, p=0.001, respectively), and CAT activity (p=0.039, p=0.024, respectively), with greater changes in subjects treated with 400 mg of CoQ10 (Table 2).

TAC, SOD, and CAT activity in seminal plasma before and after CoQ10 treatment
Furthermore, in group 1 (200 mg/day), significant positive correlations were found between sperm concentration and TAC (r=0.52, p=0.008), SOD activity (r=0.46, p=0.022), and CAT activity (r=0.41, p=0.028). Similar correlations were between sperm motility and TAC (r=0.76, p=0.001), SOD activity (r=0.54, p=0.006) and CAT activity (r=0.48, p=0.014), as well as between normal sperm morphology and TAC (r=0.37, p=0.04) and SOD activity (r=0.4, p=0.034) (Table 3). The strongest correlations were found between sperm concentration, motility, and antioxidant measures.

Correlations between semen parameters and antioxidant parameters in patients in group 1
Moreover, in group 2 (400 mg/day), significant positive correlations were found between sperm concentration and TAC (r=0.55, p=0.005), SOD activity (r=0.49, p=0.009), and CAT activity (r=0.38, p=0.02); between sperm motility and TAC (r=0.68, p=0.002), SOD activity (r=0.61, p=0.003), and CAT activity (r=0.53, p=0.005); as well as between normal sperm morphology and CAT activity (r=0.36, p=0.04) (Table 4). The strongest correlations were likewise found between sperm concentration, motility, and antioxidant measures.

Correlations between semen parameters and antioxidant parameters in patients in group 2
Discussion
The present study demonstrated that the reduced form of CoQ10 exerted beneficial effects on sperm concentration, motility, and antioxidant capacity in men with idiopathic OAT. Greater changes were detected in response to a dose of 400 mg/day. To our knowledge, this is the first study to compare the effect of two doses of CoQ10 on seminal plasma antioxidant capacity.
Our findings are consistent with previous reports. Exogenous intake of CoQ10 may increase its levels in seminal plasma and enhance sperm function [1]. Treatment with ubiquinol (100 mg twice a day) for 6 months improved sperm motility and morphology in patients with idiopathic OAT [25]. Further, in a randomized double-blind placebo-controlled clinical trial in men with men with idiopathic asthenospermia who received CoQ10 (200 mg daily) for 6 months, significant improvements were observed in all seminal parameters, along with increased CoQ10 levels in seminal plasma [1]. Similar findings were reported by Safarinejad and colleagues [16,26] after administration of CoQ10 (200 mg) for 26 weeks in men with OAT and 300 mg daily for 26 weeks in men with OAT. Balercia et al. [1,6] reported an increase in CoQ10 levels in seminal plasma and improvements in sperm parameters following administration of CoQ10 (200 mg/day) for 6 months. In contrast, in an open-label prospective study, men with OAT who were treated with CoQ10 (600 mg) for 12 months showed significant improvements in sperm progressive motility, concentration, and morphology at the 12-month follow-up [27].
Adequate CoQ10 levels are necessary for proper spermatozoa function given the role of CoQ10 in the mitochondrial respiratory chain and its antioxidant properties. In particular, mitochondrial dysfunction in spermatozoa has been associated with reduced sperm motility; and OS has been shown to be related with mitochondrial DNA deletions [28]. OS is detrimental for sperm parameters, DNA integrity, and fertilization [20]. Therefore, the improvements in sperm parameters detected in the present study could be attributed to the antioxidant properties of CoQ10, leading to reduced OS and enhanced mitochondrial reduction-oxidation function. Previous studies have also linked dietary supplementation with CoQ10 to increased levels of CoQ10 in circulating lipoproteins and enhanced resistance of human low-density lipoprotein to lipid peroxidation [29]. Increased sperm concentration and motility may enhance fertility potential and pregnancy outcomes. A body of literature has demonstrated beneficial effects of CoQ10 and other antioxidants on semen parameters. However, there is a lack of agreement on the type and the use of individual or combination antioxidant therapy [18,30]. A recent meta-analysis also showed that doses of CoQ10 varied (200–300 mg/day) [15]. In addition, a head-head comparison is not always possible due to the heterogeneity of studies in terms of methodology, patient selection, controls, and the dosing and duration of CoQ10 therapy.
The observed improvement in seminal fluid parameters in the current study was higher with a CoQ10 dose of 400 mg per day. Indeed, CoQ10 plays a central role both as an antioxidant and as a facilitator of adenosine triphosphate synthesis [8]. Thus, it is likely that a greater dose and length of exposure yield stronger effects [21]. This is supported by the meta-analysis of Lafuente et al. [3], in which pooled data from three trials revealed that CoQ10 treatment significantly enhanced multiple sperm quality parameters. The studies above also used variable doses of CoQ10 for different durations, highlighting the absence of consensus on the optimal dose for CoQ10 in infertile men. If the optimal effective dose is determined, this treatment is inexpensive, safe, and easy to administer. Furthermore, optimisation of CoQ10 dosing is essential, as recent reports indicated that excessive intake of antioxidants may shift the reduction-oxidation balance to reductive stress, which is as harmful as OS [31]. Once the positive effects of antioxidant supplementation are confirmed, it remains necessary to optimize the dose and duration of treatment and to identify which seminal parameters benefit the most from certain antioxidants. In patients experiencing high levels of OS, doses should be taken for a minimum of 3 months, as the maturation of sperm takes around 72 days. Based on this study, a 400 mg dosage of CoQ10 could be suggested as effective dosage for treatment of patients with idiopathic OAT.
In our study, we also observed enhancements of the oxidative environment, as reflected by the improvement of TAC, SOD and CAT levels, as well as the positive correlations between these variables and semen parameters after 3 months of CoQ10 treatment. Previous studies have demonstrated lower TAC, SOD and CAT levels in infertile men than in fertile men [13,32]. In addition, a meta-analysis by Huang et al. [12] reviewed studies on 3,819 male infertility patients and showed lower levels of antioxidant activity, including TAC, SOD, and CAT, in men with infertility. Previous reports have also detected an increase in antioxidant capacity following antioxidant therapy [17,33]. However, studies of the effects of CoQ10 intake on seminal plasma antioxidant levels are limited. Our findings are congruent with those of Nadjarzadeh et al. [13], who showed that CoQ10 administration (200 mg/day for 3 months) increased SOD and CAT activity in the seminal plasma of infertile men. Furthermore, a positive correlation was found between seminal CoQ10 concentrations and semen parameters [26]. In contrast, in a study by Eroglu et al. [34], basal CoQ10 levels in seminal fluid did not appear to be associated with sperm quality parameters or TAC.
The increased TAC, SOD and CAT activities in our study could partially explain the improvement in sperm parameters after treatment with CoQ10. Although CoQ10 has been recognized as a powerful mediator of cell signalling [35], no specific mechanisms have been identified concerning CoQ10-mediated upregulation of TAC and SOD and CAT activity [36]. Interestingly, CoQ10 has been observed to prevent proinflammatory signalling by insulin, interleukin-17, and STAT3 [37], as well as tumour necrosis factor alpha and various chemokines [38]. In turn, this may reflect an enhanced antioxidant status. Future investigations are needed to elucidate the mechanisms of the CoQ10-mediated enhancement of antioxidant capacity. Our study has certain limitations. We did not investigate pregnancy or live birth rates post-therapy, as those were not the primary outcome measures of the study. Dietary regulation was also not measured in this study. Other limitations include the small sample size and lack of long-term follow-up, so further large-scale long-term clinical studies are warranted.
In conclusion, treatment with CoQ10 improved sperm motility, concentration, and semen antioxidant status in infertile men with idiopathic OAT, with a greater improvement observed in response to a dose of 400 mg/day than a dose of 200 mg/day. Supplementation with CoQ10 may enhance the fertility potential and reproductive outcomes of men with idiopathic infertility.
Notes
Conflict of interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
The author would like to express sincere gratitude to all patients who participated in this study for their valuable help in carrying out this work. The author is also very grateful for Dr. Pallav Sengupta, Mahsa University College, Kuala Lumpur, Malaysia for reviewing this manuscript prior to submission.