Introduction
Infertility refers to the failure of couples to conceive after at least 1 year of unprotected coitus, and it affects 13%–18% of couples [1,2]. Female factors are responsible for nearly 30% of all infertility cases. The main reason for female infertility is ovulation dysfunction [3], which impacts around 40% of women suffering from infertility [4]. Hormone secretion is crucial to the initiation of ovulation; therefore, impairment of hormone pathways can lead to ovulation dysfunction [5,6].
An appealing treatment option for women with dysfunctional ovulation is ovulation induction, which also increases the quality and quality of oocytes for use with assisted reproductive techniques [7-9]. Several ovulation induction drugs exist, the most common of which are human menopausal gonadotropin (HMG) and clomiphene citrate [10,11]. Ovarian hyperstimulation and multiple births are the most important side effects of these medications [12-14]. The use of newer methods and a more comprehensive understanding of patients’ genetic background can play an important role in reducing the side effects of these drugs.
Follicle-stimulating hormone (FSH) [15] and luteinizing hormone (LH) [16] are the hormones most crucially involved in the regulation and initiation of ovulation [13,17]. In women, the reduced secretion of LH or FSH interferes with the reproductive cycle. Medications that regulate the levels of FSH and LH are widely used to facilitate assisted reproductive techniques [9,18]. The present study is of particular importance because if we can recognize the gene variations that affect ovulation (especially the induction of ovulation), we can use this information to design advanced infertility treatment.
The glutamate ionotropic receptor AMPA type subunit 1 (GRIA1) gene, which encodes a subunit of a ligand-gated ion channel, is located on chromosome 5q33.2 and spans 20 exons [19,20]. In humans, a strong association between the GRIA1 rs548294 C > T and rs2195450 G > A polymorphisms and migraine risk has been demonstrated in many case-control studies [19,21,22]. Moreover, GRIA1 regulates FSH and LH secretion by controlling the release of gonadotropin-releasing hormone [23]. Very few studies have investigated the association between the GRIA1 gene and infertility in humans, and most related studies have been performed in cattle [23]. In addition, studies in cattle have shown that the GRIA1 polymorphism results in the replacement of serine with asparagine. This reduces the release of gonadotropin-releasing hormone, resulting in defective ovulation [24]. Considering the findings regarding the relationship between GRIA1 genetic variants and ovulation, the purpose of the present study was to evaluate the association of the GRIA1 rs548294 C > T and rs2195450 G > A polymorphisms with the ovarian response to ovarian stimulation treatments in Iranian women.
Methods
1. Study population
This cross-sectional study was performed on 100 infertile women (age: range, 20–35 years) who had been referred to the Abortion Research Center at Yazd Reproductive Sciences Institute. The Institutional Ethics Committee of Yazd Reproductive Sciences Institute approved the study, and written informed consent was obtained from all participants. All patients were treated with long-protocol ovulation induction, and on the second day of menstruation, patients were injected with HMG. On the third day of the menstrual cycle, a blood sample was collected in a simple tube with no additive for serum extraction and evaluation of LH and FSH levels. A blood sample was also collected in an ethylenediamine tetraacetic acid (EDTA)-containing tube for the extraction of DNA and the determination of the genotype with regard to GRIA1 polymorphisms. On the ninth day of the menstrual cycle, the number of follicles was evaluated via ultrasound. Patients with a history of pelvic surgery or ovarian cyst were excluded. All patients were candidates for in vitro fertilization (IVF) for various reasons (male factor infertility, uterine malformations, or unexplained infertility) and had experienced at least 1 year of infertility.
2. Genotyping
Genomic DNA was obtained from whole blood using the Qiagen QIAamp DNA Blood Mini Kit (Cat No. 51105; Qiagen, Hilden, Germany). The quality and quantity of extracted DNA were quantified via an agarose gel and spectrophotometry (optical density 260/280), respectively. The GRIA1 rs548294 G>A and rs2195450 C>T genotypes were assessed via the polymerase chain reaction (PCR)-restriction fragment length polymorphism technique. PCR of the GRIA1 rs548294 C>T and rs2195450 G>A polymorphisms was conducted using the following primers: for the GRIA1 rs548294 C>T polymorphism, a forward primer of 5´-AGATGAAGAAACAGAGGTC-3´ and a reverse primer of 5´-CCCCAGGTACTATTCAAAG-3´; and for the rs2195450 G >A polymorphism, a forward primer of 5´- TCTAAGAGGAGGGGGCAAGG-3´ and a reverse primer of 5´- GCTTGGTAGATGGTGCTTGA-3´.
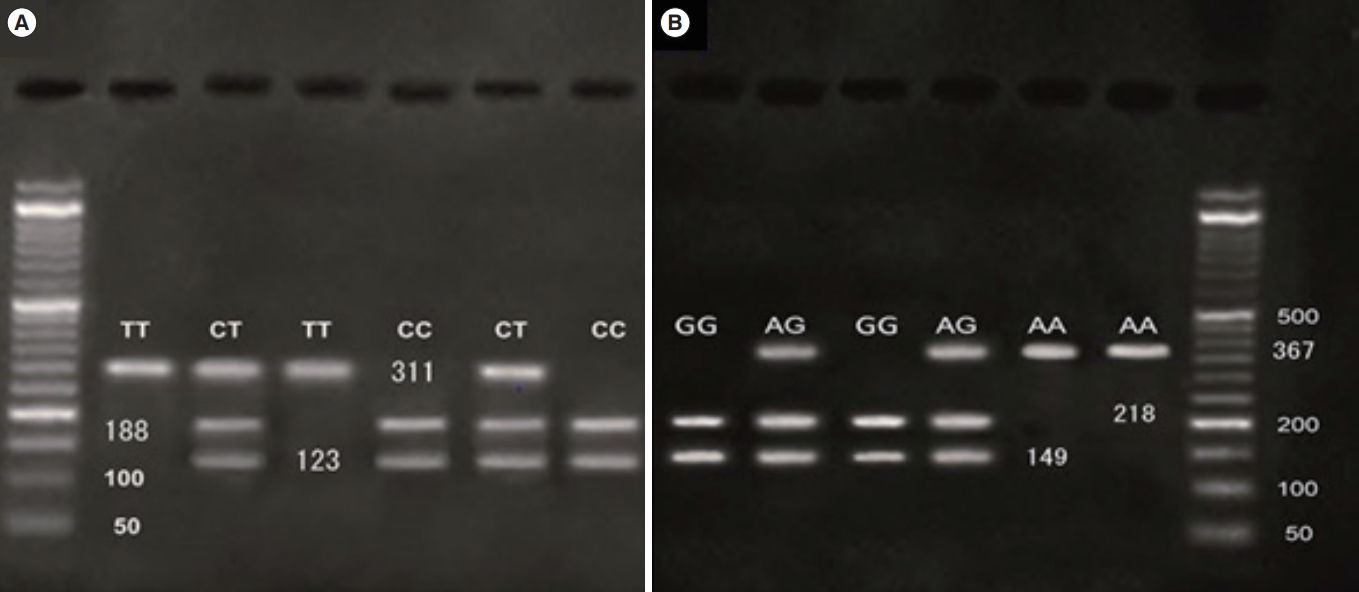
The GRIA1 rs548294 C > T and rs2195450 G > A polymorphisms were identified by digesting the PCR products with the restriction endonucleases MwoI and TaqI, respectively. An agarose 3% gel and electrophoresis were applied, and the results were immediately visualized under ultraviolet illumination for assessment of the genotypes of the specimens (Figure 1).
3. Statistical analysis
Statistical analysis was performed using SPSS ver. 18.0 (SPSS Inc., Chicago, IL, USA). Differences in allele and genotype frequencies among the patients were analyzed via the chi-square test and analysis of variance. Logistic regression was used to calculate odds ratios and 95% confidence intervals. Two-tailed p-values of less than 0.05 were considered to indicate statistical significance.
Results
1.Hormonal analysis
The mean LH and FSH levels by GRIA1 rs548294 C>T and rs2195450 G > A polymorphism genotype are presented in Tables 1 and 2, respectively. For the GRIA1 rs548294 C > T single-nucleotide polymorphism (SNP), the frequencies of genotypes CT, CC, and TT were 48%, 29%, and 23%, respectively. For the GRIA1 rs2195450 G > A SNP, the frequencies of genotypes AG, GG, and AA were 20%, 75%, and 5%, respectively. The results indicate a significant relationship between the mean levels of LH and FSH and the GRIA1 rs548294 C > T SNP; specifically, the mean LH and FSH levels associated with the CT genotype were higher than those associated with the other two genotypes (p = 0.000 for both LH and FSH). These outcomes also show a significant relationship between the mean levels of LH and FSH and the GRIA1 rs2195450 G > A SNP, with the GG genotype associated with higher levels of both LH and FSH than the other two genotypes (p = 0.029 and p = 0.000, respectively).
2.Number of follicles at day 9 of the menstrual cycle
The mean number of follicles at day 9 of the menstrual cycle by GRIA1 rs548294 C > T and rs2195450 G > A polymorphism genotype are shown in Table 3. Of the 91 patients for whom the mean number of follicles was assessed, for the GRIA1 rs548294 C > T SNP, the number of cases with genotypes CT, CC, and TT were 44, 27, and 20, respectively; for the GRIA1 rs2195450 G > A SNP, the number of cases with genotypes AG, GG, and AA were computed as 18, 68, and 5, respectively. A significant relationship was observed between the mean number of follicles at day 9 and both GRIA1 rs548294 C > T and rs2195450 G > A SNPs. Specifically, regarding the GRIA1 rs548294 C > T SNP, the mean number of follicles was higher in subjects with the CT genotype than in those with the other two genotypes (p = 0.002). Regarding the GRIA1 rs2195450 G > A SNP, the mean number of follicles was higher in subjects with the GG genotype than in those with the other 2 genotypes (p = 0.000).
3. Correlation between LH, FSH, and number of follicles
The Pearson correlation analysis showed significant positive correlations between LH and FSH levels (r = 0.504, p < 0.01), LH levels and number of follicles (r = 0.611, p < 0.01), FSH levels and age (r = 0.207, p < 0.05), number of follicles and age (r = 0.192, p = 0.048), and FSH levels and number of follicles (r = 0.438, p < 0.01). However, no significant correlation was found between LH levels and age (r = 0.162, p = 0.107) (Table 4). These results illustrate the interactions among FSH and LH levels, age, and number of follicles.
Discussion
Ovarian dysfunction occurs in approximately 15%–25% of infertility cases, and the response to treatment is typically very satisfactory when ovarian dysfunction is the only cause of infertility [25]. Briefly, successful treatment in these individuals depends on careful examination and identification of the underlying cause of ovulatory dysfunction. A reliable method to predict ovarian response to different ovarian stimulation methods would be extremely helpful in determining the prognosis of these methods with regard to pregnancy. Thus, it is necessary to consider the genetic backgrounds of individuals that may lead to varied responses to different doses of ovarian stimulation drugs.
To the best of our knowledge, this experiment was the first that assessed the association between GRIA1 rs548294 C > T and rs2195450 G > A polymorphisms and ovarian response to ovarian stimulation treatments in Iranian women. The hormonal analysis showed that, for the GRIA1 rs548294 C > T and rs2195450 G > A SNPs, respectively, the CT and GG genotypes were associated with higher mean FSH and LH levels than the other genotypes. These polymorphisms in GRIA1 lead to the replacement of serine with asparagine. GRIA1Asn has a weaker affinity for glutamate than GRIA1Ser. This replacement decreases the secretion of gonadotropin-releasing hormone, leading to defective ovulation. In cows, GRIA1 polymorphisms result in the reduced release of gonadotropin-releasing hormone and a decreased response to hormone treatment. Due to the crucial role of GRIA1 in regulating FSH and LH secretion, it is important to consider the genotypes associated with increased levels of these hormones.
The number and size of follicles are important factors in the success of assisted reproductive methods [26]. Many factors, including genetic variants, age, and hormones, contribute to follicle quality [27]. In this study, comparison of the mean number of follicles at day 9 of the menstrual cycle showed that, similarly to the mean LH and FSH levels, the number of follicles in subjects with the CT and GG genotypes was higher than in subjects with the other genotypes in the GRIA1 rs548294 C > T and rs2195450 G > A SNPs, respectively. Therefore, considering individuals’ genotype when determining appropriate doses of ovulation-stimulating drugs seems necessary.
Age is also important to consider for choosing the right treatment. Many studies have shown that levels of FSH and LH increase with age, and this increase leads to reduced ovarian reserve and decreased follicle quality [16,28]. Our results also showed significant relationships among FSH levels, LH levels, number of follicles, and age. An increase in FSH levels is a sign of decreased fertility in women, and it therefore seems reasonable that FSH levels would have prognostic value [29]. The results of the present study are consistent with other studies that have shown that increased age, and consequently increased FSH levels, lead to an increase in infertility rate and a decrease in the follicle count [30]. Conflicting results have been published regarding the relationship between LH levels and age, with some studies, such as that by Rahmani et al. [16], reporting a significant relationship. Moeini et al. [31] and Scheffer et al. [32] found a significant relationship between age and FSH concentrations, but not between age and LH levels. Separate studies also reported no significant relationship between age and LH levels [16,30]. In the present study, significant correlations were found between the follicle count and FSH levels and between the follicle count and LH levels, but no significant relationship was observed between LH levels and age.
Consequently, the present study showed a significant relationship between the GRIA1 rs548294 C >T and rs2195450 G >A polymorphisms and ovarian responses to the induction of ovulation. Considering the effect of these polymorphisms on LH and FSH secretion and hence on the ovulation process, it can be suggested that variants of the GRIA1 gene, as well as other genes that influence ovulation, can aid in the choice of treatment protocol and the administered dosage of ovulation-stimulating drugs. However, more detailed studies with larger samples are needed to confirm the results of this experiment.