Introduction
Recurrent pregnancy loss (RPL) is a major concern in reproductive medicine [1]. It is defined as more than two clinical pregnancy losses before the 20th week of gestation [2]. Various causes of RPL have been proposed, including immunological and hormonal disorders and/or genetic anomalies such as chromosomal abnormalities in embryos [3]. A recent descriptive case-control study concluded that unexplained RPL may be due to an increased frequency of abnormal sperm parameters, sperm DNA fragmentation (SDF), defective chromatin condensation, or sperm aneuploidy [4]. A recent systematic review and meta-analysis of 15 prospective studies suggested a significant association between SDF and RPL [5]. The aforementioned review showed a remarkably higher rate of SDF in the male partners of women with RPL than was found in the male partners of fertile women, with a mean difference of 11.91 (95% confidence interval, 4.97–18.86) [5].
There are two protamine genes in humans that are located on chromosome 16: PMN1, which codes for protamine P1, and PMN2, which codes for protamine P2 [6]. In human sperm cells, 85% of the histones are replaced by protamine, allowing sufficient chromatin density to be achieved [7] and reducing the availability of sites that could be harmed by DNA-damaging agents [8]. Evidence indicates that a high proportion of histones in sperm relative to protamine causes defective chromatin compaction, subsequently leading to an increased risk of male infertility [9]. A proper ratio of protamine P1 to protamine P2 (normal, 0.8–1.2) is required for normal sperm function [10]. The inappropriate expression of PMN1 and/or PMN2 [11], both at the mRNA and protein level [12], can lead to an abnormal ratio of protamine P1 to protamine P2 in infertile men. Furthermore, some reports have demonstrated that changes in the genes coding for protamines modulated substantial changes in sperm chromatin structure, resulting in failed spermatogenesis [13,14].
Sperm abnormalities, such as DNA or/and chromatin damage, can endanger the early stage of embryo development and the potential of embryos for implantation [15]. Lack of chromatin integrity, which may manifest as protamine deficiency, can influence sperm function [7] and quality [16]. Moreover, protamine deficiency can interfere with DNA protection due to the distinct importance of protamine-DNA complex stability [17].
In the human body, antioxidant systems are present in order to neutralize free radicals [18]. An imbalance between free radical production and the antioxidant capacity causes oxidative stress (OS), which affects the structure, function, and motility of spermatozoa, leading to male infertility [19,20]. Antioxidant-based dietary supplementation promotes the motility of sperm cells and appropriate sperm concentrations [19,21].
Vitamin C is a water-soluble substance that is absorbed through the small intestine [22]. Previous studies showed that effective antioxidants, such as vitamin C, are essential for the maintenance of sperm function and DNA integrity [20,23]. Moreover, vitamin C deficiency is associated with OS induction in the male reproductive system, which leads to reduced sperm production [24].
Notwithstanding the potential role of vitamin C in improving human sperm quality, no prospective trial has yet assessed the effect of vitamin C on the expression of protamine genes. Therefore, the aim of this randomized clinical trial (RCT) was to examine whether taking at least 250 mg of vitamin C daily for 90 days improved sperm parameters and the gene expression profile of protamines in the male partners of couples with RPL.
Methods
1. Participant selection
This prospective study was registered in the Iranian Registry of Clinical Trials with the national ID No. IRCT20180312039059N1. Informed consent was obtained from all participants. The participants were randomly selected among patients referred to the Yazd Research and Clinical Center for Infertility using a random number table. Twenty male partners of couples with RPL due to male factor infertility were selected as the intervention group. The control group (n=20) included the male partners of couples with no varicocele, no chronic diseases, a normal genital examination, normal sperm parameters according to the 2010 World Health Organization (WHO) criteria [25], and a child born in the last 2 years. The inclusion criteria for participants were as follows: age of less than 40 years, no history of alcohol abuse or use of any types of tobacco and/or cigarettes, no antidepressant use, a sperm concentration of 7–14 million/mL, total sperm motility <40%, and a percentage of sperm with normal morphology <4%. Obesity (based on body mass index), diabetes, and varicocele disorders were exclusion criteria. None of the included couples had been treated with antioxidants or other medications before this study. Men who were treated with other medications during the study were also excluded. In addition, a number of exclusion criteria were defined for the female partners, including the absence of a hormonal imbalance, chromosomal alterations, tubal obstruction, and bacterial or viral infections.
The intervention group was administered 250 mg of vitamin C daily in tablet form (Avicenna Co., Tehran, Iran) for 3 months by an expert urologist. The dosage of vitamin C and the duration of the intervention were set in accordance with a previous report on the efficient duration and dosage of vitamin C treatment [26]. The participants were recommended to consume fruits and vegetables regularly during their treatment, and to refrain from soft drinks, soybeans, any kind of canned food, and even unnecessary use of mobile phones and/or laptops. After 3 months, sperm parameters and chromatin were assessed in the intervention group. Moreover, pregnancy outcomes were followed in the couples who received vitamin C supplementation. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. This study was approved by the Ethics Committee of Yazd Research and Clinical Center for Infertility. In this study, all procedures were conducted by an experienced laboratory technician who was blinded to the study to the allocation of participants.
2. Hormone assessments
In order to ensure the reproductive health of the female partners of couples in the intervention group and to facilitate comparisons with the controls, levels of sex hormones in the female partners were measured at the beginning of the study. Blood samples (5 mL) were collected from all participants. Blood fractionation was done by 10 minutes of centrifugation at 2,500 ×g. Ultimately, 3 mL of the upper phase (blood serum) was separated using special enzyme-linked immunosorbent assays to measure levels of follicle-stimulating hormone (FSH), luteinizing hormone (LH), prolactin (PRL), and anti-Müllerian hormone (AMH).
3. Sperm sample collection
Semen samples were obtained by masturbation after at least 48–72 hours of sexual abstinence. Semen analysis was performed according to the 2010 WHO guidelines [27]. The specimens were prepared by the swim-up method. Half of the prepared specimens were used for morphological examinations and chromatin/DNA integrity assessments, and the other half was used to evaluate participants’ gene expression profile
4. Sperm parameters
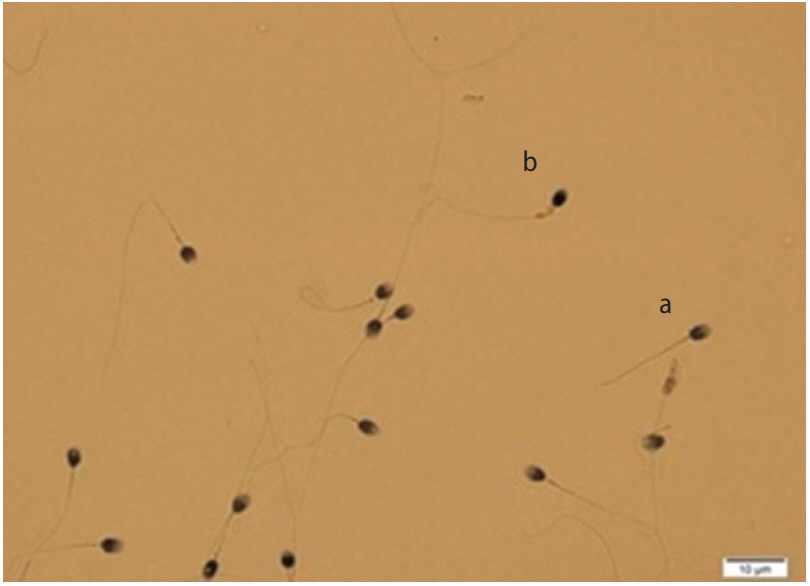
The analysis of all samples was conducted according to the WHO standard values provided in 2010 [25]. Sperm concentration and motility were determined under light microscopy at ×400 magnification. The Diff-Quik staining method was used to evaluate sperm morphology. At least 200 sperm cells were counted in each slide with a magnification of ×1,000 (Figure 1).
5. Sperm DNA integrity tests
1) Sperm protamine deficiency
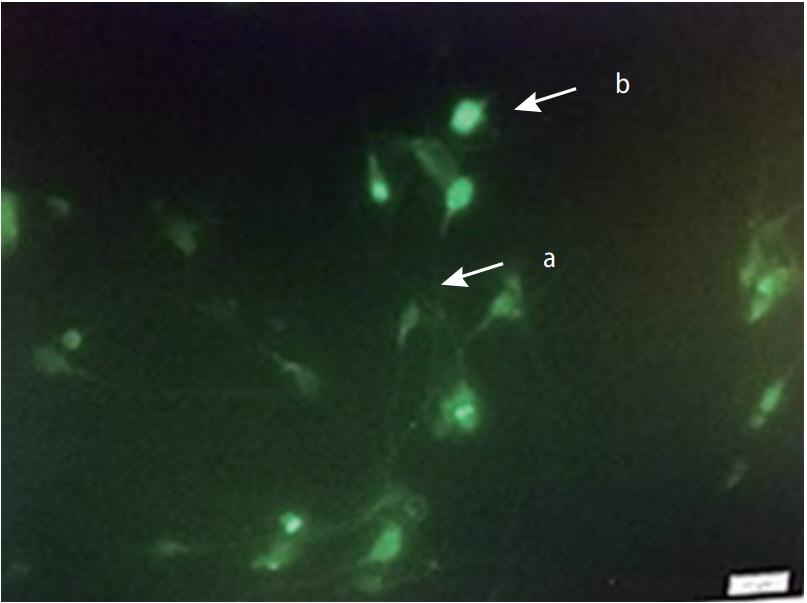
To assess sperm protamine deficiency, Carnoy solution was used to fix each sample slide for 10 minutes at 4°C. Subsequently, each slide was treated with chromomycin A3 (CMA3) solution for 10 minutes in a darkroom (Sigma-Aldrich, Sigma-Aldrich, MO, USA) and analyzed under fluorescent microscopy (×1,000 magnification) (Figure 2) [28]. Spermatozoa with protamine defects (CMA3+) were stained as bright yellow, and normal spermatozoa (CMA3–) as dark yellow.
2) Sperm DNA fragmentation
Sperm apoptosis was quantified through a terminal deoxynucleotidyl transferase dUTP nick-end labeling (TUNEL) assay using a kit (In Situ Cell Death Detection Kit with Fluorescein; Roche, Indianapolis, IN, USA). Spermatozoa with normal DNA were visualized as white, while sperm with a strong fluorescent color demonstrated increased levels of SDF (Figure 3) [27,28].
6. Protamine gene expression profile
Total RNA extraction and cDNA synthesis of all sperm samples were performed using an RNeasy Plus Universal Mini Kit (Qiagen, Hilden, Germany) and a cDNA synthesis kit (Applied Biosystems, Foster City, CA, USA), respectively, following the manufacturer’s instructions. RNA concentration and purity were detected by a NanoDrop spectrophotometer (Thermo Scientific, Waltham, MA, USA). The adjusted concentration of purified total RNA (100 ng/μL) was applied for cDNA synthesis. The relative gene expression levels of PMN1 and PMN2 were evaluated by quantitative real time-polymerase chain reaction (ABI 7300; USA) utilizing SYBR Green PCR Master Mix (Applied Biosystems). Beta-2 microglobulin (B2M) was used as the reference gene. Table 1 summarizes the primers used for all the evaluated and controlled genes (PMN1, PMN2, and B2M). The 2–ΔΔCT technique was used to present levels of gene expression normalized to those of B2M using threshold cycle (CT) values. In this method, ΔCT is defined as the CT of a target gene (here, PMN1 or PMN2) minus the CT of a reference gene (here, B2M). Then, ΔΔCT is defined as the ΔCT of a target sample minus the ΔCT of a reference sample.
7. Statistical analysis
All data were statistically analyzed using IBM SPSS ver. 23.0 (IBM Corp., Armonk, NY, USA), with p-values <0.05 considered to indicate significant differences. The paired t-test was used to analyze the data before and after the treatment. One-way analysis of variance and the Tukey test were used to analyze the differences in gene expression levels within and between the groups. The Pearson test was also used to calculate correlations.
Results
In this RCT, the male participants in the control and intervention groups were similar in terms of the demographic variables of age (33.5±1.1 vs. 35.1±1.5 years) and body mass index (25.51±1.69 vs. 25.75±1.25 kg/m2). No complications were reported at the time of vitamin C administration during the study. Before starting the treatment with an antioxidant, the mean number of abortions and the duration of infertility in women with RPL were 2.3±0.95 and 8.9±4.3 years, respectively. Furthermore, all the women with RPL had hormonal levels in the normal range, including FSH, LH, PRL, and AMH (Table 2). As summarized in Table 3, pregnancy and live birth outcomes improved after treatment with vitamin C, while the number of abortions (20%) showed a reasonable decrease in the women with RPL in the intervention group.
Sperm concentrations were significantly lower in the intervention group, both before and after treatment with vitamin C, than in the control group. However, after treatment, sperm concentrations improved in the intervention group compared to the values observed before treatment (Table 4). The proportion of normal sperm morphology was significantly lower in the intervention group than in the control group, before and after treatment. In contrast, we observed a significantly higher percentage of sperm morphology after treatment in the intervention group (Table 4). Compared to the control group, the proportion of sperm cells with protamine deficiency and apoptotic cells were remarkably higher in the intervention group before undergoing vitamin C treatment. Both before and after the administration of vitamin C, a significant difference was present between the intervention and control groups with regard to the proportion of sperm cells with apoptosis and protamine defects. However, a reasonable decrease in the number of sperm cells with positive TUNEL and CMA3 findings was observed in the intervention group after the intervention (Table 5).
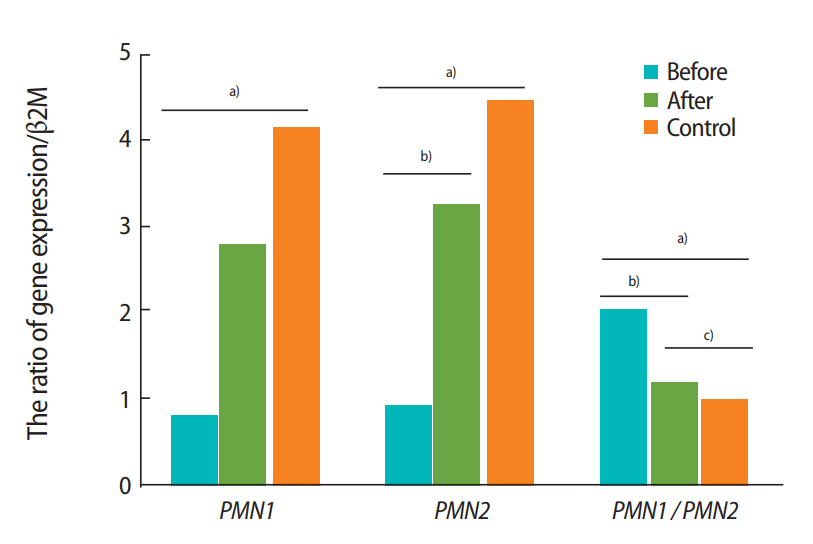
The gene expression levels of both PMN1 and PMN2 in the male partners of couples with RPL were significantly lower prior to treatment than those in the control group (by 3.9- and 4.6-fold, respectively. After taking vitamin C for 3 months, the PMN1/PMN2 ratio significantly decreased in the intervention group compared to the pretreatment values (Figure 4). As shown in Table 6, there were strong, significant, positive correlations between the expression levels of PMN1 and PMN2 (r=0.92, p<0.001).
Discussion
To evaluate the possible impacts of vitamin C on sperm parameters, chromatin and DNA integrity, and the protamine gene expression profile, 20 male partners of couples with RPL received 250 mg of vitamin C daily for 3 months in the present study. Our results indicate that a diet rich in vitamin C could significantly improve sperm morphology to the normal range (normal morphology in more than 4% of spermatozoa) in male partners (Table 4). Anbara et al. [29] also reported a positive association between vitamin C intake and sperm quality. Gil-Villa et al. [30] investigated the effect of antioxidants on sperm parameters in male partners of couples with RPL, and reported that an antioxidant-rich diet could improve sperm parameters and function, in accordance with our findings. In contrast, the beneficial effects of antioxidants on sperm parameters were not confirmed by Ko and Sabanegh [31]. Akmal et al. [32] reported increases in the percentage of sperm with normal morphology and sperm concentration in infertile men after taking vitamin C orally (1,000 mg twice daily for 2 months). Okon and Utuk [33] suggested that oral administration of vitamin C at moderate doses (250 mg) significantly increased the quality of sperm parameters, serum levels of testosterone, and the percentage of normal sperm morphology. However, we did not observe any significant changes in sperm concentration. These differences can be attributed to the use of varying doses of vitamin C and short-term consumption in different studies [21].
However, we observed an impressive effect of vitamin C on sperm chromatin quality and DNA integrity (Table 5). It is thought that semen parameters do not directly represent the status of sperm nuclei, as sperm with normal motility and morphology may have chromatin and/or DNA abnormalities [34]. Previous studies have found significant positive correlations between DNA fragmentation and CMA3 positivity in infertile men [27,28,35]. Moreover, protamine defects were associated with the fertilization rate in stimulated assisted reproduction cycles according to Bianchi et al. [36] and Iranpour et al. [37]. Deemeh et al. [38] revealed that male partners of couples with RPL had high levels of protamine deficiency. As DNA integrity plays a key role in sperm function, it can be a better predictor of sperm fertility potential than conventional sperm parameters [39]. The results of three studies conducted by Aoki et al. showed that more severe protamine deficiency was related to DNA damage in infertile men [11,14,40]. Previous research demonstrated a positive correlation between reactive oxygen species levels and apoptosis rate in seminal plasma [39,41]. Antioxidants have been observed to reduce apoptosis in testicular cells and to improve sperm quality [42]. In addition, high levels of OS can change sperm function and chromatin structure, and can induce apoptosis by altering the amount of intracellular calcium [43]. Unlike oocytes, sperm cannot repair their DNA damage. Therefore, a sperm cell with damaged DNA is condemned to have poor-quality chromatin and functional deficiencies [44]. DNA damage is not considered to be the main cause of fertilization failure, but it is expected to impair embryo development and lead to the abortion of embryos [31].
In this RCT, we observed significantly lower expression levels of each protamine in the intervention group than in the control group, both before and after the intervention. We also discovered a negative correlation between PMN1 and PMN2 mRNA levels and sperm DNA integrity (Table 6). In line with our findings, Rogenhofer et al. [45] recently conducted an observational study and reported significant differences in PMN1 and PMN2 mRNA levels and the ratio of PMN1 to PMN2 mRNA between couples with recurrent miscarriages and healthy controls (p<0.01). Despite the small sample size and ambiguity regarding the precise mechanism, they suggested that the levels of protamine gene expression in spermatozoa were not only essential for successful fertilization, but also for appropriate early embryo development [45]. In contrast, Torregrosa et al. [46] reported no relationship between PMN2 gene expression and sperm DNA integrity. Due to the associations of protamine replacement with acrosome formation and normal sperm morphology, any defects in the replacement process resulting from protamine deficiency (such as low protamine expression) may lead to sperm dysfunction, resulting in poor implantation and pregnancy outcomes [47]. We found that vitamin C could improve spermatogenesis by increasing protamine expression and chromatin condensation.
The relative expression of PMN2 significantly increased after vitamin C treatment (Figure 4), explaining the higher ratio of PMN1 to PMN2 in the intervention group than in the controls in this study. According to recent findings, the ratio of PMN1 and PMN2 expression is approximately 1:1 in healthy men, and any change in this ratio is associated with male infertility [10]. Another study showed that the PMN1/PMN2 ratio was abnormal in infertile men [48]. Additionally, it has been found that changes in PMN2 expression leading to a reduction in the mRNA levels of PMN2 may be responsible for the altered proportion of PMN1 to PMN2 in infertile men [7].
It is believed that OS may have a destructive effect on fertility in both the male and female reproductive systems [49,50]. However, the presence of antioxidants in semen can protect chromatin and/or DNA integrity against free radical damage [51]. According to a recent study, vitamin C—along with some other antioxidants such as lycopene, coenzyme Q10, zinc, and selenium—can be used to treat OS in sperm. In the aforementioned report, a daily dose of 200 mg or 1,000 mg of vitamin C was recommended according to prescriptions designed specifically to augment male fertility [52]. Our clinical findings demonstrated improvements in pregnancy outcomes, including a lower rate of pregnancy loss and increased rates of clinical pregnancy and take-home babies (Table 3). In a case series, male partners were instructed to consume a diet rich in antioxidants or commercial multivitamins containing beta-carotene, vitamin C, vitamin E, and zinc for at least 3 months. In that study, all male partners of couples with a history of recurrent embryo loss who received antioxidant supplementation achieved successful pregnancy [30]. Vitamin C is known to be an important antioxidant for reducing sperm abnormalities and protecting sperm DNA from OS [29]. It is also required for normal spermatogenesis and sperm function [53]. Yun et al. [54] reported that vitamin C could significantly decrease lipid peroxidation and increase glutathione peroxidase levels. Consequently, in their study, it increased testosterone concentration and the spermatid population. The current RCT was the first attempt to investigate the potential impacts of antioxidants on protamine expression, at both the gene and protein levels, in the male partners of couples with RPL, and we suggest that further clinical trials should be carried out with larger populations and with assessments of the efficacy of other antioxidants.
In conclusion, our findings demonstrated a remarkable increase in protamine gene expression after treatment with vitamin C. It seems that daily oral administration of vitamin C can improve human sperm parameters and DNA integrity by increasing protamine gene expression levels in the male partners of couples with RPL. The beneficial effects of vitamin C supplementation as an antioxidant for the male partners of couples with RPL could lead to improved pregnancy outcomes in these cases.