The features of the reproductive population in South Korea have been changing: the mean age at first marriage has reached the 30s; the mean age at first pregnancy was 32.2 years in 2015; and those ages have increased continuously (Korean Statistical Information Service, Statistics Korea, 2015). In 2014, the Ministry of Health and Welfare of the Republic of Korea reported that the total number of women with subfertility or infertility had reached 210,000 up from 170,000 in 2007. With the increase in maternal age and the number of infertile women undergoing assisted reproductive interventions, the incidence of reproductive failure, including recurrent pregnancy loss (RPL) and repeated implantation failure (RIF), is increasing.
For a successful pregnancy, the maternal immune system must maintain a balance between defense against microorganisms and accommodation toward a fetus [1]. Immune abnormalities have been reported as an etiology of RPL, RIF, and other pregnancy complications [2,3,4]. Cellular immune abnormalities have been reported in women experiencing reproductive failure, including increased natural killer (NK) cell levels, altered T helper (Th)1/Th2 cell ratios, altered Th17/regulatory T cell ratios, or NK cytotoxicity [1,2,3,4,5,6,7,8]. In addition, the prevalence of antiphospholipid antibodies (APAs) was as high as 20% in women with RPL and 30% in women with RIF [9,10,11,12].
Intravenous immunoglobulin G (IVIG) is derived and purified from the plasma of 3,000 or more donors and contains more than 95% unmodified immunoglobulin G. Since the first demonstration of the effectiveness of IVIG in the treatment of immune thrombocytopenia purpura in 1981 [13], it has been widely used to treat autoimmune and inflammatory diseases, and it was introduced as an intervention for women with RPL in 1991 [14,15,16,17,18]. The immunomodulatory effects of IVIG are mediated through two different portions of the immunoglobulin. The F(ab┬┤)2-dependent mechanisms include the killing of target cells by antibody-dependent cytotoxicity, the blockade of cell-cell interactions mediated by cell-surface receptors such as Fas and Fas ligand (CD95L), the neutralization of cytokines and autoantibodies, and the scavenging of the anaphylatoxins C3a and C5a. The Fc-dependent mechanisms include the saturation of the neonatal Fc receptor, the expansion of regulatory T cell populations, the blockade of immune complex binding to activating Fc╬│ receptors, the modulation of dendritic cell activation via Fc╬│ receptor III, and the modulation of activating and inhibitory Fc╬│ receptor expression on innate
immune effector cells and B cells.
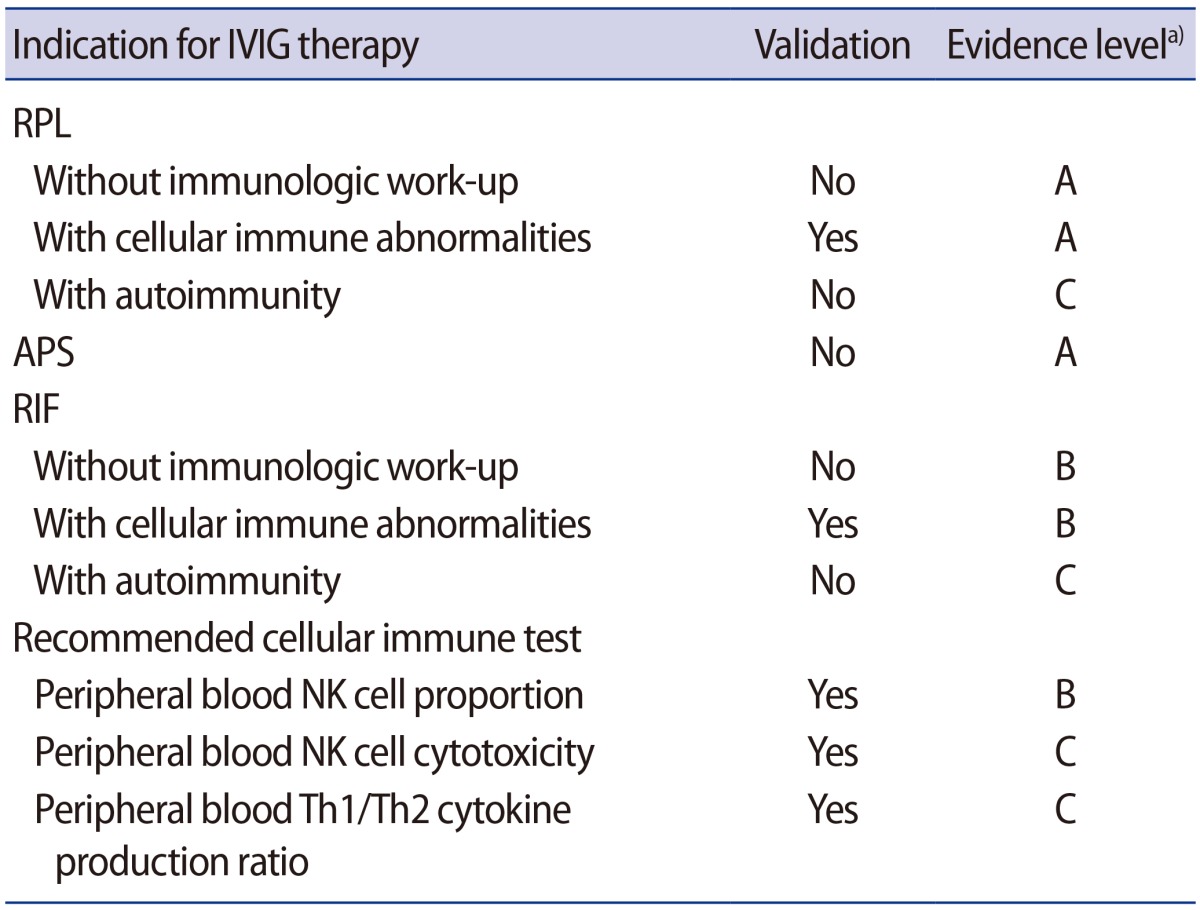
Although the evaluation of cellular immune factors in women with reproductive failure is becoming more popular, appropriate cut-off values for the tests have not yet been established, and remedies for those abnormalities are still controversial. Even though a meta-analysis of IVIG for women with RPL and randomized controlled trials have not demonstrated a beneficial effect [19,20,21], IVIG is commonly prescribed for women with reproductive failure. However, there is no consensus on the indication and treatment protocol for IVIG in those women. Thus the Korean Society for Reproductive Immunology launched the IVIG Task Force to establish IVIG treatment guidelines for women experiencing reproductive failure (Table 1).
The validity of IVIG therapy for each indication
We reviewed the relevant scientific papers investigating the clinical efficacy of IVIG for reproductive failure, with a publication date up to September 31, 2016, by searching PubMed, and we determined indications for IVIG treatment for reproductive failure patients. Each indication was classified and assigned a level according to power of the evidence: a level A classification requires at least one randomized control trial as part of a body of literature of overall good quality and consistency that addresses the specific recommendation; level B requires the availability of well-controlled clinical studies, but no randomized control trials on the topic of the recommendation; and level C requires evidence obtained from expert reports of the opinions and/or clinical experiences of respected authorities, indicating an absence of directly applicable clinical studies of good quality [22].
1. Unexplained RPL
Although RPL has been traditionally defined as three or more consecutive miscarriages [23], the American Society for Reproductive Medicine Practice Committee Opinion defined RPL as two or more failed pregnancies, based on the risk of recurrence and the prevalence of etiologies [24,25]. Unexplained RPL has been defined as those cases without identifiable genetic, uterine, endocrine, infectious, or autoimmune factors [26]. After systematic evaluation, more than half of cases of RPL were classified as unexplained [27]. Several meta-analyses of randomized clinical trials of IVIG therapy for unexplained RPL failed to prove its effectiveness [20,21,28].
Empirical IVIG treatment in women with unexplained RPL is not recommended (evidence level A).
2. RPL in women with cellular immune abnormalities
Kwak et al. [29] showed that the use of IVIG in patients with RPL effectively suppressed elevated peripheral blood NK cells (CD56+, CD56+/16+), and 86.3% of women with RPL who had elevated NK cell counts had a successful pregnancy outcome after IVIG and anti-coagulation treatment. Graphou et al. [30] reported favorable effects of IVIG on Th1/Th2 imbalance in women with RPL. Another study also showed that IVIG modifies the Th1/Th2 balance during early pregnancy (4ŌĆō5 gestational weeks) in women with RPL without other etiologies [31]. IVIG was also effective in reducing the increased peripheral blood NK cell counts and/or NK cell activities in women with unexplained RPL [32,33,34]. Moraru et al. [35] reported that IVIG improved the live-birth rate in women with reproductive failure who had high levels of NK cells. Recently, Lee et al. [36] demonstrated that the live-birth rate was significantly higher in cases of idiopathic RPL in women with cellular immune abnormalities treated with IVIG than in cases of idiopathic RPL in women who were not treated with IVIG, as reported in other studies (82% vs. 42%). The possible mechanisms of action of IVIG in RPL are (1) the neutralization of cytotoxic antibodies, (2) the downregulation of NK cell numbers and activity, (3) the regulation of Th1/Th2 balance, and (4) the expansion of regulatory T cell populations [33,37,38].
IVIG treatment is recommended for women who have RPL with cellular immune abnormalities (evidence level A).
3. RPL in women with APAs
A prospective randomized trial reported that low-molecular-weight heparin (LMWH) with low-dose aspirin (LDA) therapy resulted in a higher live-birth rate than IVIG therapy in women with RPL and APAs (84% vs. 57%) [39]. Dendrinos et al. [40] showed consistent results (LMWH with LDA, 72.5% vs. IVIG, 39.5%; p=0.003). Although IVIG has a neutralizing effect for cytotoxic antibodies, the efficacy of IVIG in women with RPL and APAs is not clear based on the published clinical data. In addition, a meta-analysis showed that IVIG treatment had no significant effect on the live-birth rate in women with RPL and APAs [41].
LMWH with LDA should be considered as the standard therapy in cases of RPL with APAs or classic antiphospholipid syndrome (APS), and IVIG is not recommended (evidence level A). However, IVIG could be considered as an alternative treatment in women who suffer side effects from heparin and/or aspirin, or in cases where those medications are contraindicated (evidence level C) [42,43].
4. Unexplained RIF
RIF is on the rise in the infertile population undergoing in vitro fertilization cycles. Currently, RIF is defined as pregnancy failure even after at least three cycles of embryo transfers of good-quality embryos [44]. Proposed mechanisms for RIF include embryo or endometrial factors, as well as decreased endometrial receptivity, which could be related to uterine anomalies, endometriosis, hydrosalpinx, and thrombophilia [45,46]. Empirical therapy strategies with aspirin and heparin showed no benefit for cases of unexplained RIF [47,48,49]. A randomized clinical trial showed that immunological treatment with IVIG did not improve the live-birth rate in cases of unexplained RIF [50]. Subsequently, a meta-analysis reviewing 10 studies reported that IVIG improved pregnancy outcomes for repeated in vitro fertilization or intracytoplasmic sperm injection failure and unexplained infertility [51]; however, this study included RIF groups both with and without immune abnormalities [35,50,52,53,54,55].
IVIG treatment in cases of unexplained RIF without immune evaluation is not recommended (evidence level A).
5. RIF in women with cellular immune abnormalities
The etiologies of RIF overlap with those of RPL, and women who have RIF may experience RPL as well. Increased peripheral blood NK cell counts and NK cell activity were reported in these cases of reproductive failure [56,57,58], as well as unfavorable Th1-oriented changes to NK and NK T-like cells [59]. Thum et al. [56] showed that IVIG suppressed the increased NK cell cytotoxicity in women with a history of RPL or RIF and Heilmann et al. [53] reported that IVIG was beneficial in cases of RIF with high NK cell levels. Moraru et al. [35] also supported the efficacy of IVIG in women with RIF and high levels of NK or NK T-like cells. Subsequently, Winger et al. [60] reported that IVIG significantly improved IVF success rates in subfertile women with increased Th1/Th2 ratios and/or NK cell levels as compared to those who did not undergo the treatment. Another observational study reported that IVIG treatment improved clinical pregnancy and live-birth rates in selected RPL and RIF patients with immunologic alterations [61].
In cases of RIF with cellular immune abnormality, IVIG treatment can be considered (evidence level B).
6. RPL or RIF with autoimmunity
Approximately 20% of women with RPL have autoimmune issues, including APAs and other autoimmune abnormalities such as anti-nuclear antibodies or thyroid autoantibodies [9,62,63]. As contributing factors for infertility and poor pregnancy outcomes, type 1 diabetes mellitus, systemic lupus erythematosus, rheumatoid arthritis, and other autoimmune disease were reviewed by Carp et al. [64]. One study suggested high-dose IVIG as a safe and effective therapy for pregnant women who had systemic lupus erythematosus and RPL with or without APS [65], but other studies showed that IVIG did not provide a significant benefit in women with APS and/or systemic lupus erythematosus [39,66]. IVIG could improve the disease activity of systemic lupus erythematosus, but there is not enough evidence supporting IVIG use for RPL or RIF patients with autoimmune diseases (evidence level C).
Evaluation for cellular immunity in RPL and/or RIF
The reported cut-off values of peripheral blood NK cell proportions in cases of reproductive failure differed across studies. Several studies regarded NK cell proportion levels over 12% of peripheral blood mononuclear cells as the cut-off for high NK cell levels, which were associated with poor reproductive outcomes [67]. Another study defined the proportion as over 12.5% [68]. A detailed analysis of cut-off values in cellular immune markers for Korean women with RPL defined proportions of NK cells of over 16.1% as abnormal [8]. A study done in Australia considered abnormal NK cell proportions as >18% [68].
NK cell cytotoxicity is due to the capability of NK cells to lyse other tissues and is measured as the percentage of target cells killed after co-culture with NK cells in vitro [69]. Lee et al. [8] determined the cut-off values of NK cell cytotoxicity and the Th1/Th2 cytokine-producing CD4 cell ratio; the optimal threshold levels of NK cell cytotoxicity were 34.3% at an effector-to-target cell (E:T) ratio of 50:1, 23.8% at an E:T ratio of 25:1, and 9.6% at an E:T ratio of 12.5:1; in addition, the cut-off value of tumor necrosis factor-alpha/interleukin 10 (TNF-╬▒/IL-10)-producing Th cell ratio was 36.2, and it was reported that IVIG therapy improved the live-birth rate in women with RPL and cellular immune abnormalities at or above these cut-off values equally well as in women with RPL without immune abnormalities [36]. Winger et al. [60] showed a significantly improved in vitro fertilization success rate with IVIG in subfertile women with increased Th1/Th2 ratios and/or NK cell counts with the following cut-off values; >30.6 for TNF-╬▒/IL-10 ratios, >20.5 for interferon-╬│/IL-10, and >12% for NK cells.
To evaluate the cellular immune abnormalities in women with reproductive failure, tests for (1) peripheral blood NK cell proportion (evidence level B), (2) NK cytotoxicity (evidence level C), and (3) Th1/Th2 cytokine cell ratios (evidence level B) are recommended (Table 1).
Regimen of IVIG in indicated patients
As the half-life of IVIG is 18 to 25 days, it is adequate to administer IVIG every 3 to 4 weeks. To minimize the side effects, the dose of IVIG and infusion rate need to be carefully controlled [70]. The recommended protocol for IVIG is as follows: (1) 400 mg/kg per each treatment, (2) every 3 to 4 weeks, and (3) from the early stage of pregnancy in women with RPL or from the beginning of the in vitro fertilization cycle for RIF patients (evidence level C). The end-point of IVIG treatment and the need for further laboratory tests can be determined by the clinician's decision, depending on the patient's state.
Prior to IVIG infusion in all patients, the blood level of immunoglobulin A must be determined and renal function tests are required. Anaphylactic reactions were reported in immunoglobulin A-deficient patients (<7 mg/dL) with IVIG, and renal insufficiency can be caused by a sugar stabilizer of IVIG that has been associated with high-dose IVIG treatment [71,72,73]. Mild side effects such as fever, malaise, myalgia, and headache were reported in 4% of patients, and myocardial infarction, renal failure, alopecia, aseptic meningitis, and renal necrosis were described as possible severe side effects [74,75,76]. However, with the proper regimen of IVIG in well-selected patients, the occurrence of side effects is very rare.
Data on IVIG treatment in neonates are abundant and there is no report of significant side effects [76,77,78]. Antenatal treatment for fetal neonatal alloimmune thrombocytopenia with maternal IVIG was not associated with lymphocyte activation or premature maturation of the neonatal immune system [79]. In addition, during the past 20 years there have been no reports of significant side effects in mothers or their babies for IVIG use prior to conception and during pregnancy. However, published studies regarding the safety of the fetus with maternal IVIG therapy during pregnancy are lacking, and longitudinal observational studies are needed.