Evaluation of sperm protamine deficiency and apoptosis in infertile men with idiopathic teratozoospermia
Article information
Abstract
Objective
Sperm morphology plays an important role in infertility, especially in cases of defects in the heads of spermatozoa. Tapered-head or elongated-head spermatozoa are examples of morphological abnormalities. The aim of this study was to compare the semen parameters, levels of protamine deficiency, and frequency of apoptosis between patients with normozoospermia and those with teratozoospermia with tapered-head spermatozoa.
Methods
Fifty-two semen samples (27 patients with tapered-head sperm and 25 fertile men) were collected and semen analysis was performed according to the World Health Organization criteria for each sample. Protamine deficiency and the percentage of apoptotic spermatozoa were evaluated using chromomycin A3 (CMA3) staining and terminal deoxynucleotidyl transferase dUTP nick-end labelling (TUNEL) assays, respectively.
Results
Sperm concentration, motility, and normal morphology in the tapered-head spermatozoa (cases) were significantly lower than in the normozoospermic samples (controls). CMA3-reactive spermatozoa (CMA3+) in the case group were more common than in the controls. Apoptotic spermatozoa (TUNEL-positive) were significantly more common in the cases than in the controls.
Conclusion
This analysis showed that tapered-head spermatozoa contained abnormal chromatin packaging and exhibited a high rate of apoptosis, which can be considered to be an important reason for the impaired fertility potential in teratozoospermic patients with tapered-head spermatozoa.
Introduction
Half of infertility cases are related to male factors, and 30% are limited to male factor infertility [1]. The first step of male infertility assessment is seminal fluid analysis, which consists of a sperm count and an analysis of motility and morphology, which provide valuable information on a patient's fertility status. Abnormalities in each of mentioned parameters are referred to oligozoospermia, asthenozoospermia, and teratozoospermia, respectively, as well as azoospermia [23]. Sperm morphology is an important semen parameter, and is considered to be a reliable index of the quality of spermatogenesis and subsequent fertility [4]. Human sperm morphological defects include a wide variety of unusual sperm shapes in the head, neck, midpiece, and tail. Previous studies have documented a relationship between abnormal sperm morphology and fertility potential [5]. The cut-off value for the normality of sperm morphology is 4% according to the last version of the World Health Organization (WHO) criteria [6]. Teratozoospermia is expressed as the percentage of atypical sperm phenotypes present in a sample, which is a good predictor for male fertility with or without the use of assisted reproductive technology [789]. Tapered-head spermatozoa are considered to have a sperm morphological defect caused by a temporary defect in Sertoli cell ectoplasmic specialization and the acroplaxome involved in nuclear formation [10].
However, spermatogenesis is a unique and complicated process, in which 80% to 85% of histones are replaced by protamine in human spermatozoa, and only 15% to 20% of testicular histones remain intact. Intermolecular and intramolecular disulphide bond formation in sperm protamines cause chromatin condensation and morphological changes in spermatids, leading to the formation of mature and differentiated spermatozoa with condensed nuclei that exhibit normal head morphology [11]. It is clear that S-S bonds are essential for sperm chromatin stability, and any reduction in S-S bonds due to protamine deficiency makes the chromatin more susceptible to denaturation [12]. Previous studies have reported a significant relationship between morphological defects in spermatozoa and their DNA integrity [131415].
To the best of our knowledge, there are insufficient data on the evaluation of sperm chromatin abnormalities in patients with tapered-head spermatozoa. Thus, the aim of the present study was to investigate the possible relationship between sperm protamine deficiency and the rate of apoptosis in the percentage of tapered-head sperm cells in infertile men.
Methods
1. Patients
In this case-control study, semen samples were collected from 52 men referred to our andrology lab at the Research and Clinical Center for Infertility in Yazd, Iran. The patients were recruited between August 2015 and February 2016. The patients were divided into two groups: 27 teratozoospermic infertile patients comprised the case group and 25 normozoospermic fertile men comprised the control group. A comprehensive evaluation to establish the aetiology of infertility was conducted, including a physical examination, smoking history, cytogenetic tests, and immunological and reproductive hormonal assays. The inclusion criteria for patients were the presence of 40% to 100% of sperm cells with tapered-head morphology (at least two times less wide than the normal shape) in their semen. An infertile man was defined as a man who had no child after a period of unprotected intercourse of more than 1 year. A control group included fertile donors who had fathered at least one child during the past 12 months and had normal semen parameters according to the 2010 WHO criteria [16]. Heavy smokers (more than a pack of cigarettes per day during the past year), drug addicts, alcohol consumers, men with history of varicocele, and men aged more than 45 years were excluded from the study. This study was approved by the ethics committee of the Yazd Research and Clinical Center for Infertility, and informed consent forms were signed by all participants.
2. Semen analysis
Semen samples were collected by masturbation after 2 to 5 days of sexual abstinence. Each specimen was allowed to undergo liquefaction, and then was evaluated for sperm concentration, motility, and morphology according to the 2010 WHO criteria [16]. Briefly, sperm motility was assessed manually by phase-contrast microscopy (Axiostar Plus; Zeiss, Göttingen, Germany) at ×400 magnification, with sperm classified as showing progressive motility (grade A), non-progressive motility (grade C), or being immotile (grade D). Papanicolaou staining was applied to evaluate morphological abnormalities, and at least 200 sperm cells were examined per slide. Sperm count was assessed using a Makler counting chamber (Sefi Medical, Haifa, Israel) [17]. All analyses were performed by a single experienced laboratory technician blinded to the study protocol.
3. Chromomycin A3 staining
Chromomycin A3 (CMA3) (Sigma, St. Louis, MO, USA) is a fluorochrome specific for guanosine and cytosine-rich sequences, and is used to evaluate the degree of protamination of chromatin in sperm [17]. At least 200 spermatozoa were counted under fluorescence microscopy (BX51; Olympus, Tokyo, Japan) with a 460-nm filter and ×100 eyepiece magnification. The percentages of spermatozoa with bright yellow heads (CMA3+) and without brightness (CMA3−) were determined and reported as percentages [18].
4. TUNEL assays
The percentage of apoptotic spermatozoa in each sample was determined by terminal deoxynucleotidyl transferase dUTP nick-end labelling (TUNEL) assays using an In Situ Cell Death Detection kit (Roche Diagnostics, Mannheim, Germany) under fluorescent microscopy; normal DNA was detected as light green and damaged DNA was seen as bright green [19].
5. Statistical analysis
SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA) was used for all data analysis. Data were expressed as mean±standard deviation. Differences between variables with a normal distribution were analysed using the Student t-test and abnormally distributed data were assessed using the nonparametric Mann-Whitney U test. A p-value <0.05 was considered to indicate statistical significance.
Results
In this research, a total of 52 semen samples were studied in two groups. The mean age was 35.41±6.5 years in cases and 34.36±5.4 years in the control group.
1. Sperm parameters
Sperm parameters, including sperm count, motility (rapid [grade A], slow [grade B], non-progressive [grade C], or immotile sperm [grade D]), and sperm morphology, in the two groups are presented in Table 1. Sperm count, motility (grades A, B, C), total motility, and sperm morphology were significantly lower in the cases than in the controls (p<0.003). Immotile sperm (grade D) were significantly less common in the control group (p<0.001).
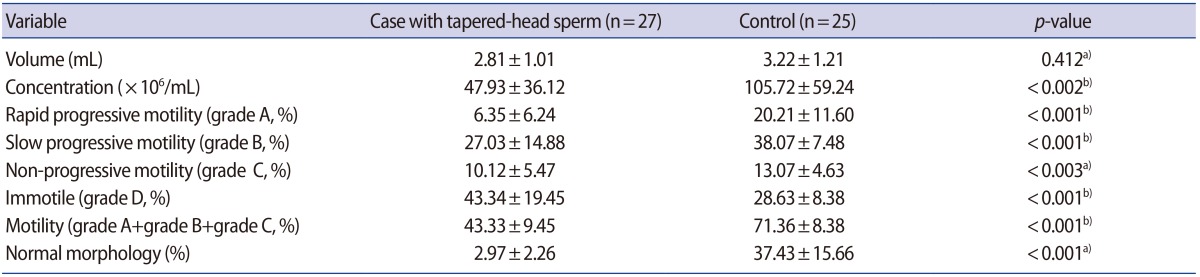
Mean and standard deviation of sperm parameters in the case and control groups
2. Assessment of sperm protamination
CMA3 fluorescent staining indicated a significant difference between the two groups (p<0.001). The mean percentage of sperm with protamine deficiency (CMA3+) was 38.7%±15.25% in the cases, compared to 23.03%±7.55% in the controls (Table 2, Figure 1).

Percentages of sperm protamine deficiency and apoptosis in the case and control groups
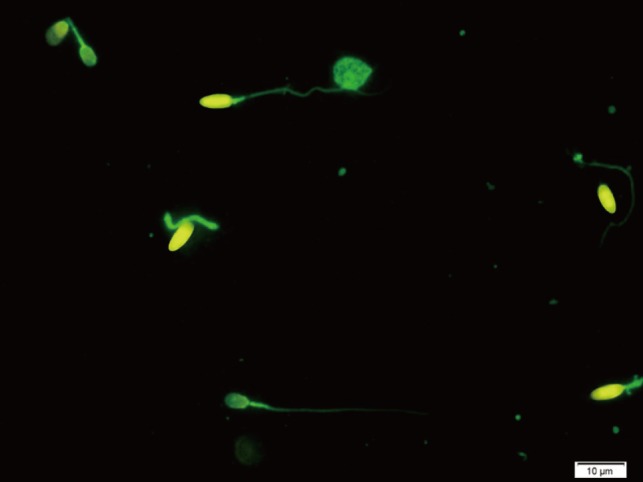
Chromomycin A3 (CMA3) staining for the evaluation of sperm protamine deficiency. Bright yellow tapered-head sperm cells (CMA3+) show protamine deficiency, and yellowish-green tapered-head sperm cells (CMA3−) show normal protamine content (fluorescence microscopy, ×100 eyepiece magnification).
3. Evaluation of sperm apoptosis
In the sperm apoptosis assessment, after TUNEL assays and the application of fluorescent microscopy, the percentage of apoptotic sperm (TUNEL+) was found to be 42.57%±18.02% and 9.03%±2.94% in the case and control groups, respectively, which was a significant difference (p=0.004) (Table 2, Figure 2).
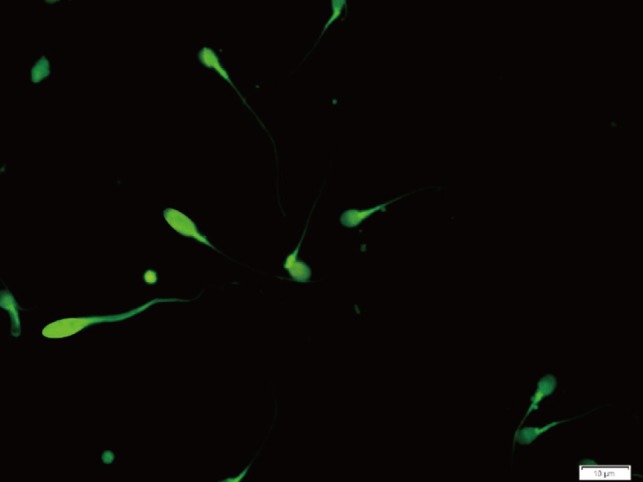
TUNEL assay for the detection of sperm apoptosis. Under fluorescent microscopy, normal DNA (non-apoptotic sperm) is seen as light green, and damaged DNA (apoptotic sperm) is seen as bright green (×100 eyepiece magnification). TUNEL, terminal deoxynucleotidyl transferase dUTP nick-end labelling.
The Pearson correlation test indicated that there was no significant relationship between semen parameters and sperm chromatin integrity or sperm apoptosis in the cases.
Discussion
Abnormal sperm morphology is correlated with nuclear chromatin integrity and consequent infertility [13]. In this study, we assessed protamine deficiency and sperm apoptosis in infertile men with tapered-head spermatozoa using CMA3 and TUNEL assays. We hypothesized that tapered-head sperm would have higher rates of protamine deficiency and apoptosis. The results showed significant differences between the two groups regarding sperm protamine deficiency. In agreement with our findings, it has been reported that DNA fragmentation was significantly more common in tapered-head sperm than in fertile controls. The TUNEL assay, which was applied in this study, has been used to show that the incidence of round-headed sperm was positively correlated to the level of DNA fragmentation. In addition, sperm with tapered heads have been directly correlated to round-headed sperm [10]. Similarly, a previous study demonstrated that the morphology of sperm selected for intracytoplasmic morphologically selected sperm injection was associated with DNA integrity, as determined using a sperm chromatin dispersion test [15]. Mangiarini et al. [14] described multiple sperm morphological defects and their correlation with the DNA fragmentation index using high-power magnification. As they documented, sperm with a vacuolated head, non-oval head, or a tapered head had a different DNA fragmentation index than morphologically normal sperm. Furthermore, tapered sperm were less likely to show positive results on a TUNEL test than vacuolated-head or small non-oval-head spermatozoa. Moreover, DNA fragmentation has been reported to be an important factor affecting sperm quality. Sperm DNA defects have been proven to have a negative effect on fertilization, implantation, embryo development, and even the health of offspring both in vivo and in vitro [2021]. In fact, the injection of sperm with abnormal morphology, including an atypical head, elongated head, or amorphous cytoplasmic droplets has been found to lead to the formation of low-fertility-potential embryos, as well as low implantation and pregnancy rates [1522].
Regarding apoptosis, we found a significantly higher rate of TUNEL-positive spermatozoa in tapered-head sperm than in normal samples. There is a negative relationship between TUNEL-positive cells and semen parameters, sperm fertilization potential, and embryo cleavage [23]. In our study, the TUNEL assay revealed a significant difference in the apoptosis rate between tapered-head and normal sperm. It has previously been reported that the most TUNEL-positive sperm with DNA fragmentation have defects in the head morphology [24]. Previous studies have also reported that the expression of apoptosis-regulated proteins was increased in pyriform sperm [25]. This may be due to abnormalities in spermiogenesis. Spermiogenic flaws may lead to germ cell apoptosis, resulting in defects in sperm count motility and morphology known as oligo-astheno-teratozoospermia (OAT syndrome) [26]. Furthermore, some antibodies can induce apoptosis and consequent chromatin defects in somatic cells, and these antibodies have been found more than twice as often in OAT patients in comparison with normozoospermic men [27]. Moreover, high concentrations of reactive oxygen species in morphologically abnormal semen samples resulted in elevated nuclear DNA damage [28] and increased apoptosis [29]. Sakkas et al. [30] showed that increased levels of TUNEL-positive spermatozoa and Fas and p53 expression were more common among men with low sperm concentration and poor morphology. In contrast, sperm nuclear DNA protection is not favourable in abnormal semen samples due to the nuclear remodelling process. One of the factors responsible for sperm DNA damage is seminal reactive oxygen species elevation [3132] in patients with leucocytosis, varicocele, and endogenous inflammation. This is also associated with abnormal sperm morphology [33], and antioxidant therapy could be beneficial for reducing reactive oxygen species-induced injuries and may provide an increased likelihood of fertility [34].
In conclusion, our study using CMA3 and TUNEL tests demonstrated a significant increase in sperm DNA protamine deficiency as well as in the apoptosis rate in patients with tapered-head sperm, and these forms of damage may affect the quality of the ejaculated spermatozoa and decrease their fertility potential both in natural cycles and in assisted reproductive technology cycles.
Acknowledgments
The authors especially thank Jalal Ghasemzadeh for his technical assistance during this research. This work was adapted from the master's student thesis.
Notes
This work financially supported by the Research and Clinical Center for Infertility, Yazd Reproductive Sciences Institute, Yazd, Iran.
Conflict of interest: No potential conflict of interest relevant to this article was reported.